Department of Pediatrics, Chang-Gung Memorial Hospital, Chiayi County, Taiwan.
College of Medicine, Chang Gung University, Taoyuan, Taiwan.
Sci Rep. 2024 Jun 3;14(1):12674. doi: 10.1038/s41598-024-63598-4.
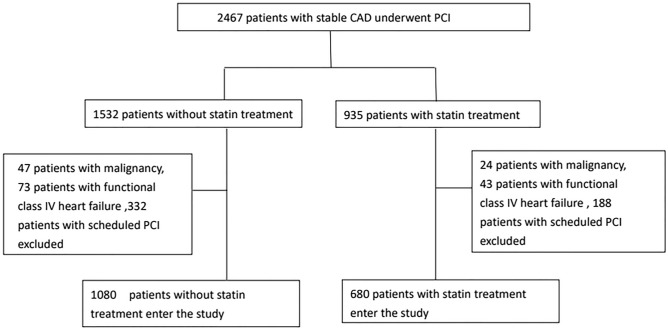
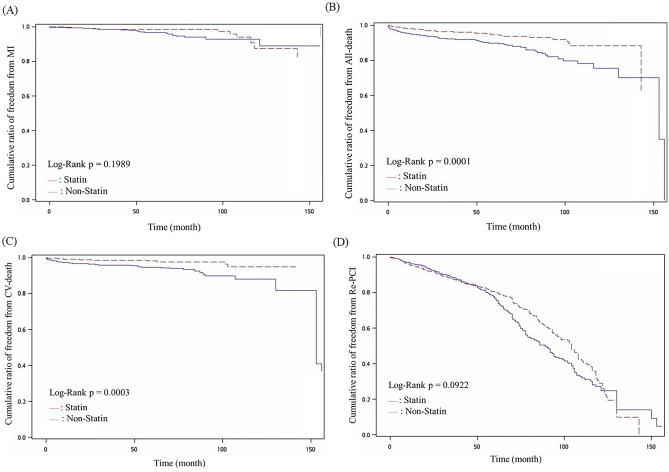
This longitudinal cohort study examined the long-term effect of statin therapy on clinical outcomes in patients undergoing percutaneous coronary intervention (PCI). A total of 1760 patients with stable coronary artery disease (CAD) were divided by receipt of statin therapy or not after index PCI. Baseline clinical characteristics, risk factors, angiographic findings, and medications after interventional procedure were assessed to compare long-term clinical outcomes between groups. Predictors for all-cause death and major adverse cardiovascular events (MACE), including myocardial infarction (MI), cardiovascular death, and repeated PCI procedures, were also analyzed. The statin therapy group had higher average serum cholesterol and more elevated low-density lipoprotein cholesterol (LDL-C) than the non-statin therapy group (189.0 ± 47.9 vs 169.3 ± 37.00 mg/dl, 117.2 ± 42.6 vs 98.7 ± 31.8 mg/dl, respectively, both P < 0.001). The non-statin group had higher rates of all-cause death and cardiovascular death compared to statin group (both P < 0.001). After adjustment for age, diabetes, and chronic kidney disease, Cox proportion hazard analysis revealed statin use significantly reduced all-cause death and repeated PCI procedure (hazard ratio: 0.53 and 0.69, respectively). Statin use seemed not reduce the hazard of cardiovascular death or MI in patients with stable CAD after PCI; however, statin therapy still was associated with reduced rates of all-cause death and repeat PCI procedure.
本纵向队列研究考察了他汀类药物治疗对经皮冠状动脉介入治疗(PCI)患者临床结局的长期影响。共纳入 1760 例稳定性冠状动脉疾病(CAD)患者,根据 PCI 后是否接受他汀类药物治疗分为两组。评估了两组患者的基线临床特征、危险因素、血管造影结果和介入治疗后的药物治疗情况,以比较长期临床结局。还分析了全因死亡和主要不良心血管事件(MACE)的预测因素,包括心肌梗死(MI)、心血管死亡和再次 PCI 术。他汀类药物治疗组的平均血清胆固醇和低密度脂蛋白胆固醇(LDL-C)水平均高于非他汀类药物治疗组(189.0±47.9 与 169.3±37.00 mg/dl,117.2±42.6 与 98.7±31.8 mg/dl,均 P<0.001)。非他汀类药物组的全因死亡和心血管死亡发生率均高于他汀类药物组(均 P<0.001)。在校正年龄、糖尿病和慢性肾脏病后,Cox 比例风险分析显示,他汀类药物的使用显著降低了全因死亡和再次 PCI 术的风险(风险比分别为 0.53 和 0.69)。在 PCI 后稳定性 CAD 患者中,他汀类药物的使用似乎并未降低心血管死亡或 MI 的风险;然而,他汀类药物治疗仍与全因死亡和再次 PCI 术的发生率降低相关。