Andersen Nicholas D, Overbey Douglas M, Prabhu Neel K, McCrary Andrew W, Sherwin Jennifer I, Allareddy Veerajalandhar, Turek Joseph W
Department of Cardiothoracic Surgery, University of Texas Southwestern and Children's Health, Dallas, Tex.
Department of Surgery, Duke Children's Pediatric & Congenital Heart Center, Duke Children's Hospital, Durham, NC.
JTCVS Tech. 2024 Feb 19;24:150-163. doi: 10.1016/j.xjtc.2024.02.006. eCollection 2024 Apr.
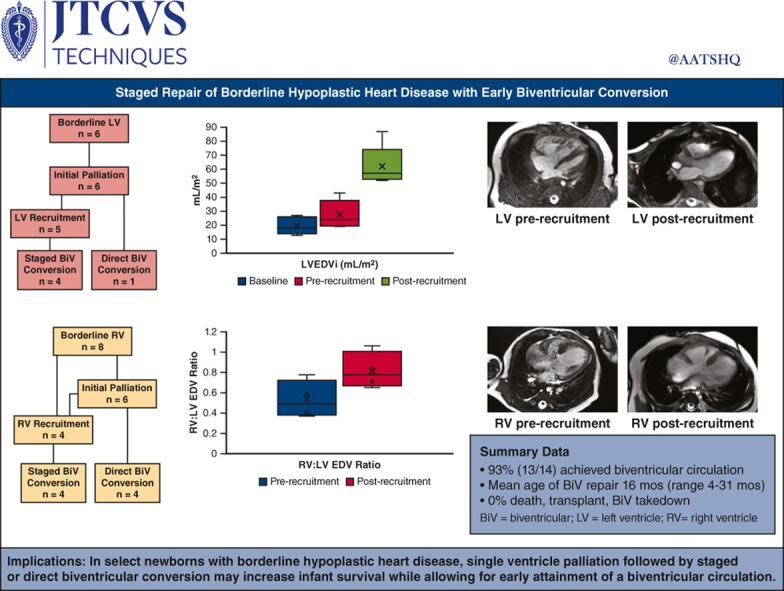
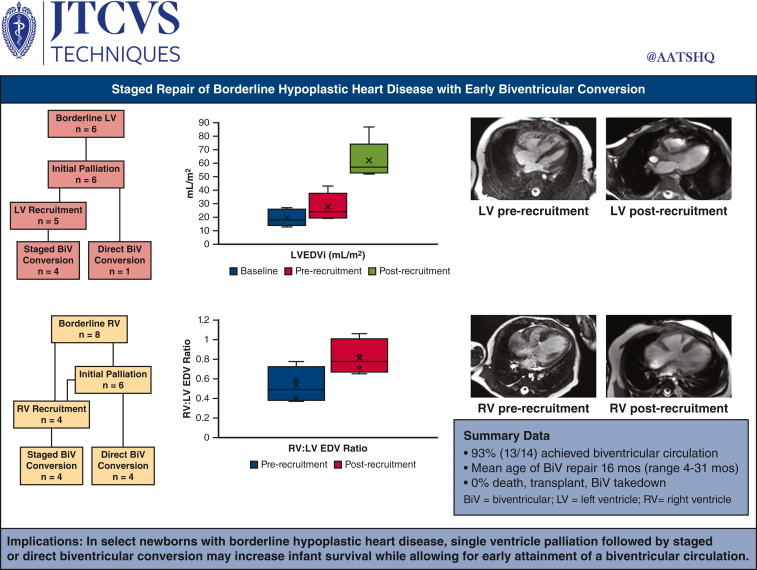
In select patients with borderline ventricular hypoplasia, we adopted a strategy of initial single-ventricle palliation followed by staged or direct biventricular conversion by 2 years of age.
Between 2018 and 2023, 14 newborns with borderline hypoplastic heart disease deemed high risk for primary biventricular repair underwent palliative procedures as a neonate/infant, followed by staged or direct biventricular conversion.
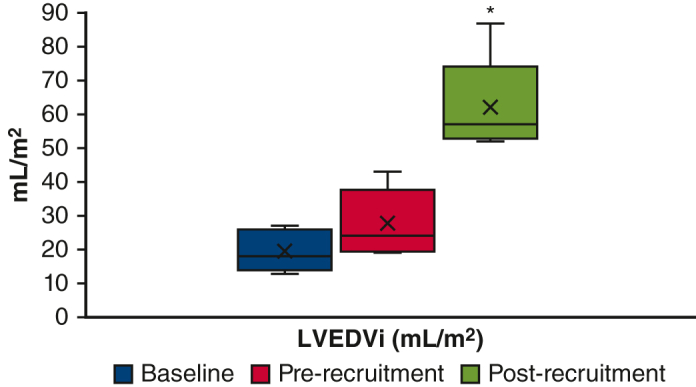
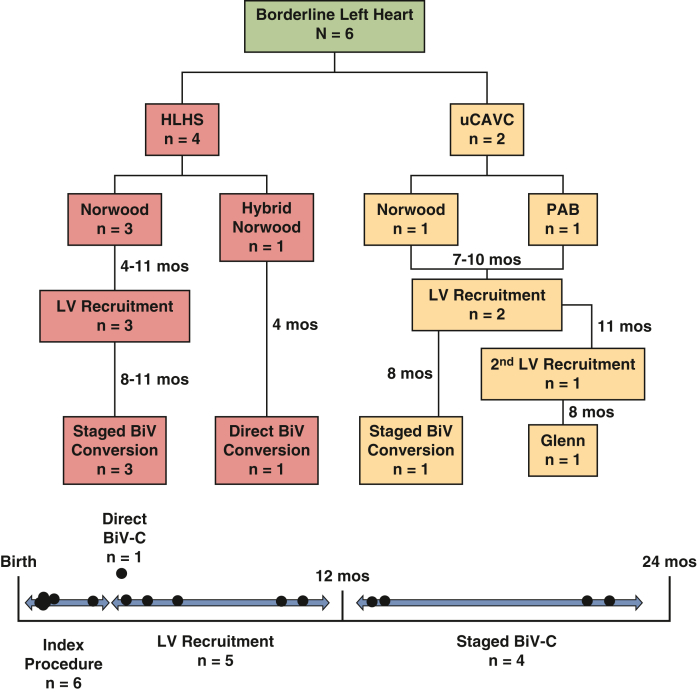
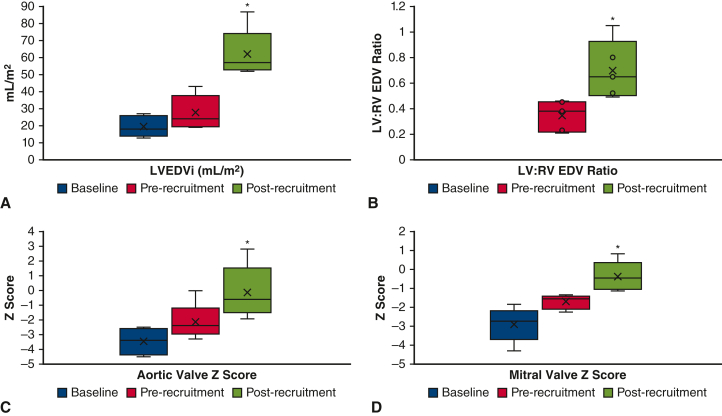
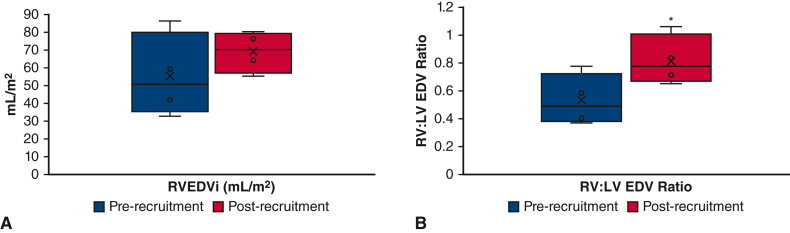
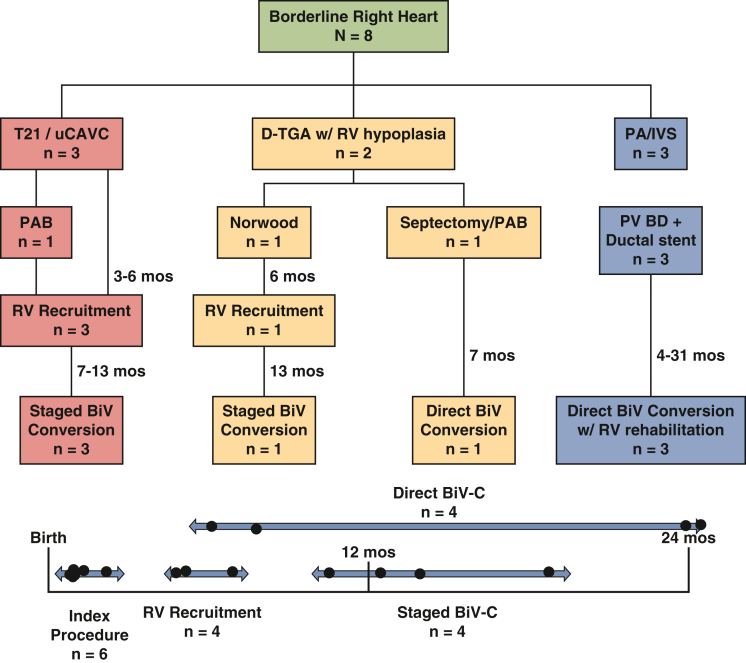
Of the 14 patients, 6 had borderline left ventricles and 8 had borderline right ventricles. Index neonatal operations were performed in 12 patients and included the Norwood operation (n = 5), pulmonary artery band (n = 3), ductal stent (n = 3), and hybrid Norwood (n = 1). Five patients underwent direct biventricular conversion, and the remaining 9 patients underwent staged ventricular recruitment operations at a mean age of 6 months (range, 3-11 months). Ventricular recruitment operations included atrial septation with or without ventricular rehabilitation, atrioventricular valve repair, or outflow tract operations. At a mean duration of 8 months (range, 4-10 months) after ventricular recruitment, there was a significant increase in chamber volume, aortic valve, and mitral valve size in patients with borderline left ventricles, and a normalization of the right ventricle:left ventricle end-diastolic volume ratio in patients with borderline right ventricles. To date, 13 of 14 patients have undergone successful biventricular conversion at a mean age of 16 months (range, 4-31 months).
In select newborns with borderline hypoplastic heart disease, single-ventricle palliation followed by staged or direct biventricular conversion may increase infant survival while allowing for early attainment of a biventricular circulation.
对于部分临界性心室发育不全的患者,我们采用了一种策略,即先进行单心室姑息治疗,然后在2岁前进行分期或直接双心室转换。
在2018年至2023年期间,14例被认为进行一期双心室修复风险高的临界性发育不全性心脏病新生儿在新生儿期/婴儿期接受了姑息治疗,随后进行分期或直接双心室转换。
14例患者中,6例为临界性左心室,8例为临界性右心室。12例患者进行了首次新生儿手术,包括诺伍德手术(n = 5)、肺动脉环扎术(n = 3)、导管支架置入术(n = 3)和杂交诺伍德手术(n = 1)。5例患者进行了直接双心室转换,其余9例患者平均在6个月(范围3 - 11个月)时进行了分期心室扩大手术。心室扩大手术包括有或无心室康复的房间隔造口术、房室瓣修复或流出道手术。在心室扩大术后平均8个月(范围4 - 10个月)时,临界性左心室患者的心室容积、主动脉瓣和二尖瓣大小显著增加,临界性右心室患者的右心室与左心室舒张末期容积比恢复正常。迄今为止,14例患者中有13例在平均16个月(范围4 - 31个月)时成功进行了双心室转换。
对于部分临界性发育不全性心脏病新生儿,先进行单心室姑息治疗,然后进行分期或直接双心室转换,可能提高婴儿生存率,同时能早期实现双心室循环。