Klarenbach Scott W, Collister David, Wiebe Natasha, Bello Aminu, Thompson Stephanie, Pannu Neesh
Department of Medicine, University of Alberta, Edmonton, Canada.
Can J Kidney Health Dis. 2024 Jun 10;11:20543581241255781. doi: 10.1177/20543581241255781. eCollection 2024.
While historical rate of decline in kidney function is informally used by clinicians to estimate risk of future adverse clinical outcomes especially kidney failure, in people with type 2 diabetes the epidemiology and independent association of historical eGFR slope on risk is not well described.
Determine the association of eGFR slope and risk of clinically important outcomes.
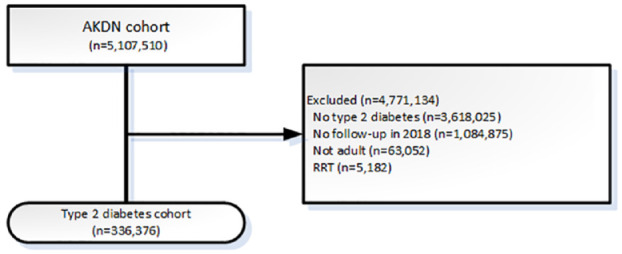
Observational population-based cohort with type 2 diabetes in Alberta.
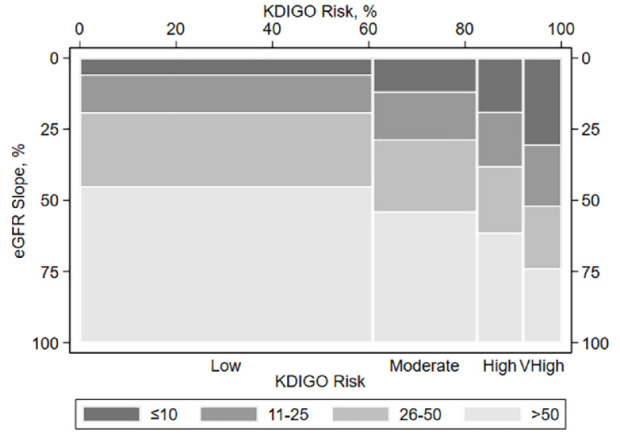
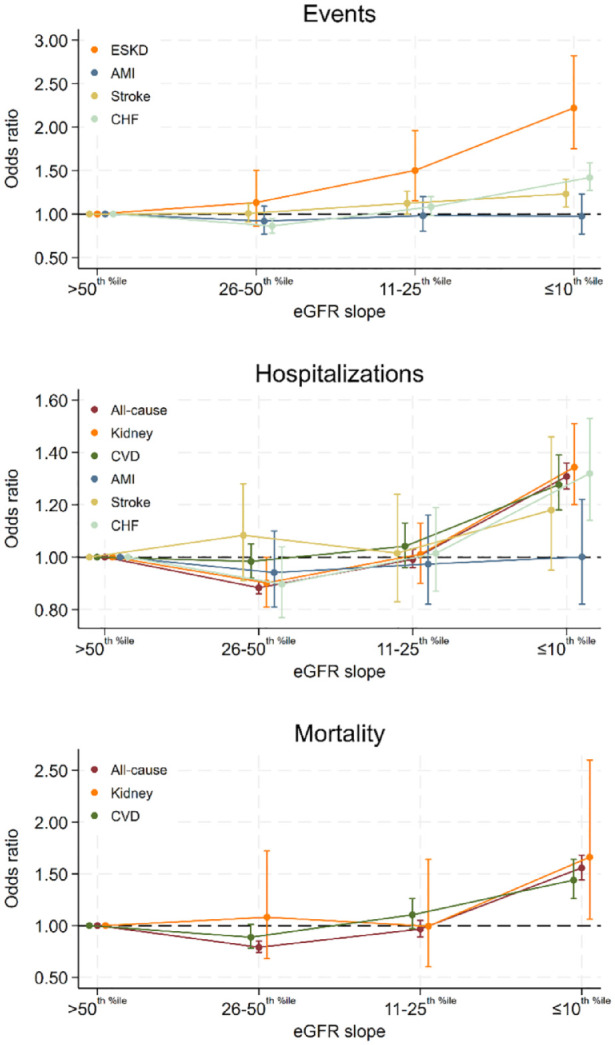
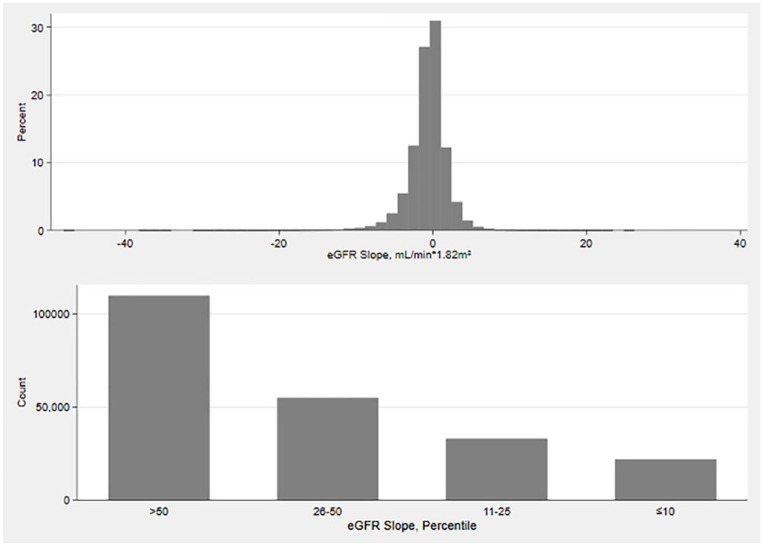
An Alberta population-based cohort with type 2 diabetes was assembled, characterized, and observed over 1 year (2018) for clinical outcomes of ESKD, first myocardial infarction, first stroke, heart failure, and disease-specific and all-cause hospitalization and mortality. Kidney function was defined using KDIGO criteria using the most recent eGFR and albuminuria measured in the preceding 18 months; annual eGFR slope utilized measurements in the 3 years prior and was parameterized using three methods (percentiles, and linear term with and without missingness indicator). Demographics, laboratory results, medications, and comorbid conditions using validated definitions were described. In addition to descriptive analysis, odds ratios from fully adjusted logistic models regressing outcomes on eGFR slope are reported; the marginal risk of clinical outcomes was also determined.
Among 336 376 participants with type 2 diabetes, the median annual eGFR slope was -0.41 mL/min/1.73 m (IQR -1.67, 0.62). In fully adjusted models, eGFR slope was independently associated with many adverse clinical outcomes; among those with ≤10th percentile of slope (median -4.71 mL/min/1.73 m) the OR of kidney failure was 2.22 (95% CI 1.75, 2.82), new stroke 1.23 (1.08, 1.40), heart failure 1.42 (1.27, 1.59), MI 0.98 (0.77, 1.23) all-cause hospitalization 1.31 (1.26, 1.36) and all-cause mortality 1.56 (1.44, 1.68). For every -1 mL/min/1.73 m in eGFR slope, the OR of outcomes ranged from 1.01 (0.98, 1.05 for new MI) to 1.09 (1.08, 1.10 for all-cause mortality); findings were significant for 10 of the 13 outcomes considered.
Causality cannot be established with this study design.
These findings support consideration of the rate of eGFR decline in risk stratification and may inform clinicians and policymakers to optimize treatment and inform health care system planning.
虽然临床医生会非正式地使用肾功能下降的历史速率来估计未来不良临床结局尤其是肾衰竭的风险,但在2型糖尿病患者中,历史估算肾小球滤过率(eGFR)斜率的流行病学及其与风险的独立关联并未得到充分描述。
确定eGFR斜率与具有临床重要意义的结局风险之间的关联。
设计、地点和患者:基于人群的阿尔伯塔省2型糖尿病观察性队列研究。
组建了一个基于阿尔伯塔省人群的2型糖尿病队列,对其进行特征描述,并在1年(2018年)内观察终末期肾病(ESKD)、首次心肌梗死、首次中风、心力衰竭以及疾病特异性和全因住院及死亡等临床结局。肾功能根据改善全球肾脏病预后组织(KDIGO)标准,使用前18个月测量的最新eGFR和蛋白尿来定义;年度eGFR斜率利用前3年的测量值,并通过三种方法(百分位数,以及带有和不带有缺失指标的线性项)进行参数化。使用经过验证的定义对人口统计学、实验室检查结果、药物治疗和合并症进行了描述。除了描述性分析外,还报告了将结局回归到eGFR斜率的完全调整逻辑模型的比值比;还确定了临床结局的边际风险。
在336376名2型糖尿病参与者中,年度eGFR斜率的中位数为-0.41 mL/min/1.73m(四分位间距-1.67,0.62)。在完全调整的模型中,eGFR斜率与许多不良临床结局独立相关;在斜率处于≤第10百分位数(中位数为-4.71 mL/min/1.73m)的人群中,肾衰竭的比值比为2.22(95%可信区间1.75,2.82),新发中风为1.23(1.08,1.40),心力衰竭为1.42(1.27,1.59),心肌梗死为0.98(0.77,1.23),全因住院为1.31(1.26,1.36),全因死亡为1.56(1.44,1.68)。eGFR斜率每降低-1 mL/min/1.73m,结局的比值比范围从1.01(新发心肌梗死为0.98,1.05)到1.09(全因死亡为1.08,1.10);在所考虑的13种结局中有10种结果具有显著性。
本研究设计无法确定因果关系。
这些发现支持在风险分层中考虑eGFR下降速率,这可能会为临床医生和政策制定者优化治疗以及为医疗保健系统规划提供参考。