Division of Medical Oncology, Department of Medical and Surgical Sciences for Children and Adults, University Hospital of Modena, Largo del Pozzo 71, Modena, 41124, Italy.
Division of Medical Oncology, Department of Oncology and Hematology, University Hospital of Modena, Modena, Italy.
BMC Cancer. 2024 Jun 15;24(1):735. doi: 10.1186/s12885-024-12506-0.
The addition of pertuzumab (P) to trastuzumab (H) and standard chemotherapy (CT) as neoadjuvant treatment (NaT) for patients with HER2 + breast cancer (BC), has shown to increase the pathological complete response (pCR) rate, without main safety concerns. The aim of NeoPowER trial is to evaluate safety and efficacy of P + H + CT in a real-world population.
We retrospectively reviewed the medical records of stage II-III, HER2 + BC patients treated with NaT: who received P + H + CT (neopower group) in 5 Emilia Romagna institutions were compared with an historical group who received H + CT (control group). The primary endpoint was the safety, secondary endpoints were pCR rate, DRFS and OS and their correlation to NaT and other potential variables.
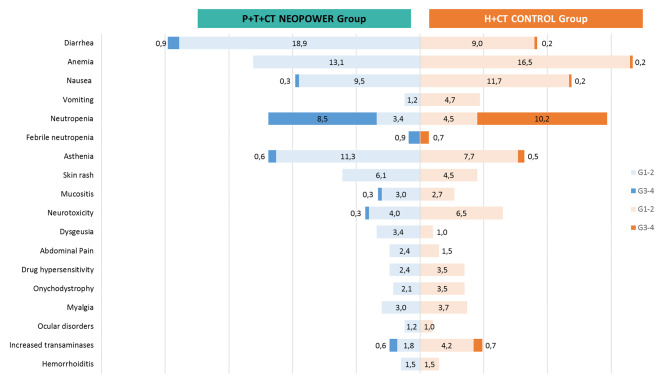
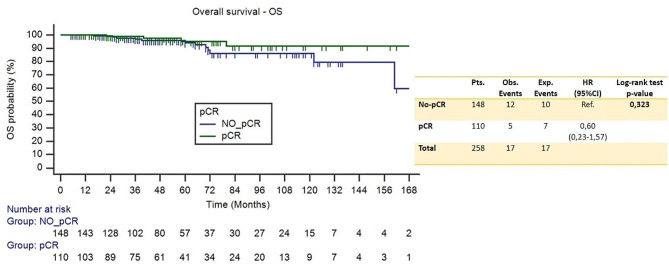
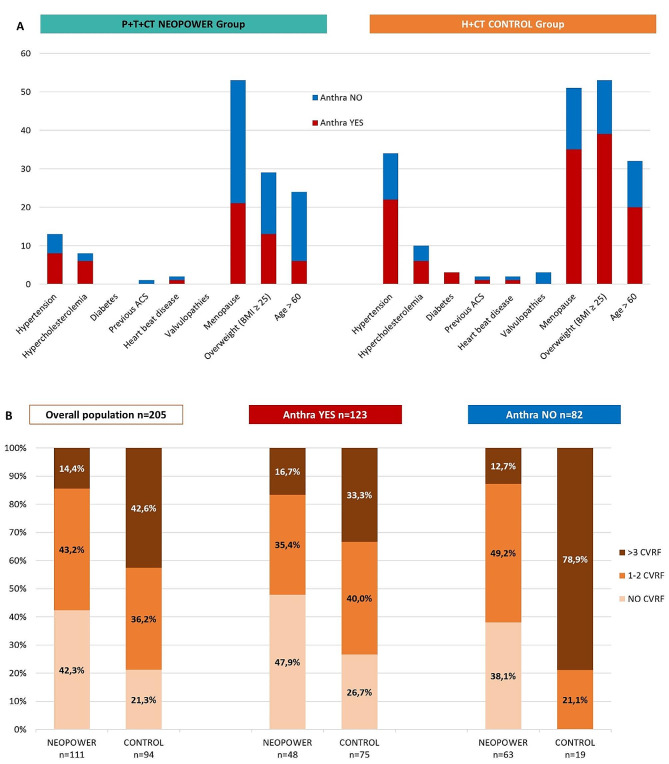
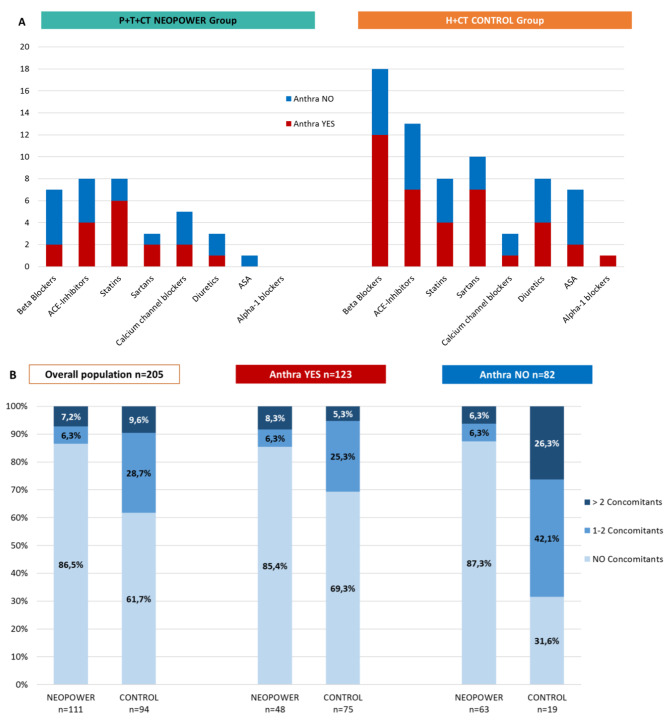
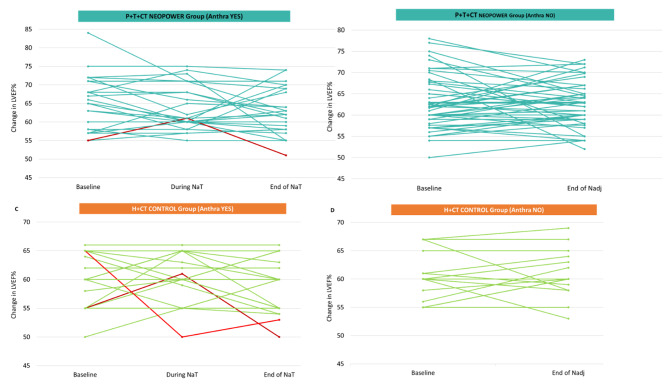
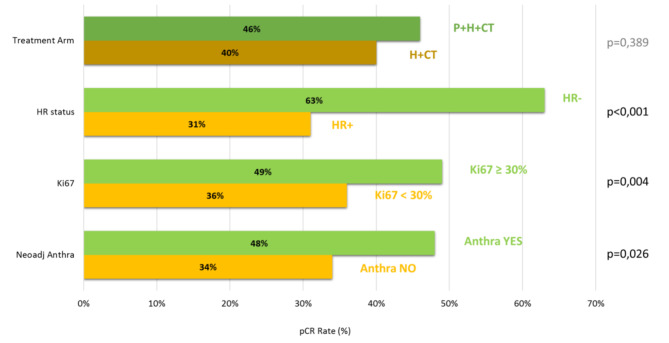
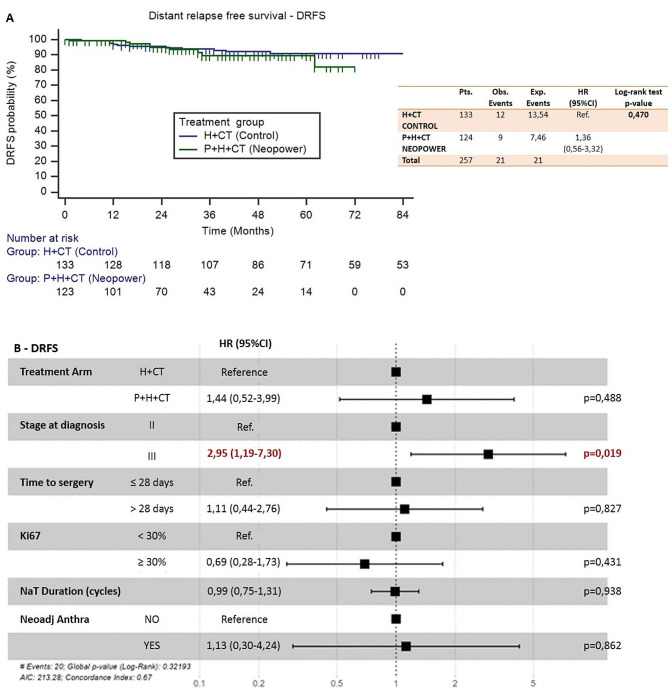
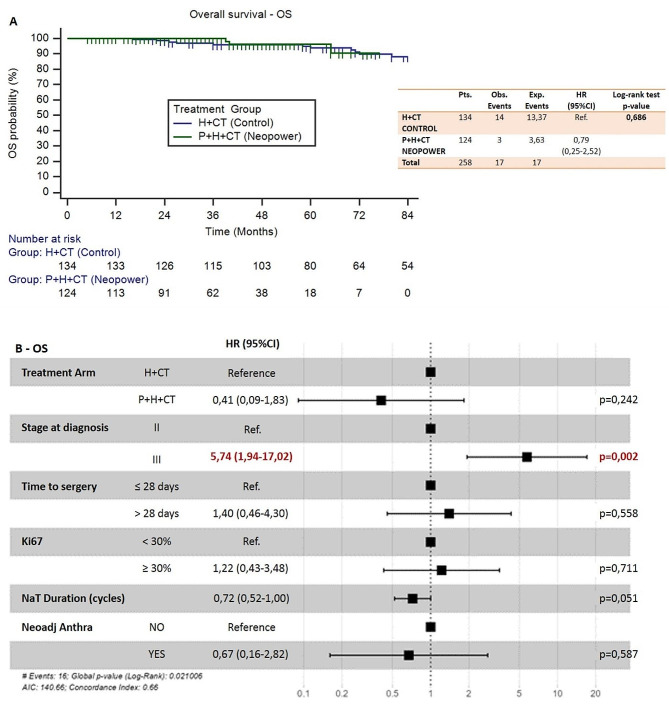
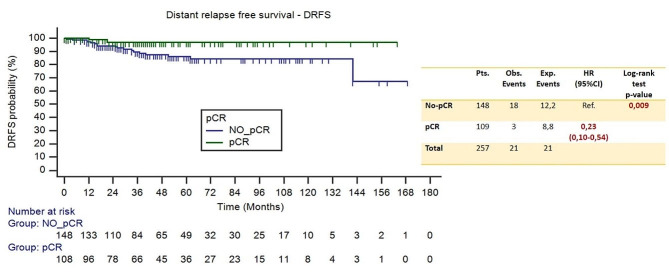
260 patients were included, 48% received P + H + CT, of whom 44% was given anthraciclynes as part of CT, compared to 83% in the control group. The toxicity profile was similar, excluding diarrhea more frequent in the neopower group (20% vs. 9%). Three patients experienced significant reductions in left ventricular ejection fraction (LVEF), all receiving anthracyclines. The pCR rate was 46% (P + H + CT) and 40% (H + CT) (p = 0.39). The addition of P had statistically correlation with pCR only in the patients receiving anthra-free regimens (OR = 3.05,p = 0.047). Preoperative use of anthracyclines (OR = 1.81,p = 0.03) and duration of NaT (OR = 1.18,p = 0.02) were statistically related to pCR. 12/21 distant-relapse events and 14/17 deaths occurred in the control group. Patients who achieve pCR had a significant increase in DRFS (HR = 0.23,p = 0.009).
Adding neoadjuvant P to H and CT is safe. With the exception of diarrhea, rate of adverse events of grade > 2 did not differ between the two groups. P did not increase the cardiotoxicity when added to H + CT, nevertheless in our population all cardiac events occurred in patients who received anthracycline-containing regimens. Not statistically significant, higher pCR rate is achievable in patients receiving neoadjuvant P + H + CT. The study did not show a statistically significant correlation between the addition of P and long-term outcomes.
曲妥珠单抗(H)联合帕妥珠单抗(P)和标准化疗(CT)作为人表皮生长因子受体 2(HER2)阳性乳腺癌(BC)的新辅助治疗(NaT),已显示可提高病理完全缓解(pCR)率,且无主要安全性问题。NeoPowER 试验旨在评估 P+H+CT 在真实世界人群中的安全性和疗效。
我们回顾性分析了在 5 家艾米利亚-罗马涅地区机构接受 NaT 治疗的 II-III 期 HER2 阳性 BC 患者的病历资料:接受 P+H+CT(NeoPower 组)的患者与接受 H+CT(对照组)的患者进行比较。主要终点为安全性,次要终点为 pCR 率、无病生存率(DRFS)和总生存率(OS),及其与 NaT 和其他潜在变量的相关性。
共纳入 260 例患者,其中 48%接受了 P+H+CT,其中 44%接受了 CT 中的蒽环类药物,而对照组为 83%。毒性谱相似,NeoPower 组腹泻更为常见(20% vs. 9%)。3 例患者出现左心室射血分数(LVEF)显著降低,均接受了蒽环类药物治疗。pCR 率分别为 46%(P+H+CT)和 40%(H+CT)(p=0.39)。仅在接受无蒽环类药物方案的患者中,P 的添加与 pCR 具有统计学相关性(OR=3.05,p=0.047)。术前使用蒽环类药物(OR=1.81,p=0.03)和 NaT 持续时间(OR=1.18,p=0.02)与 pCR 相关。对照组中有 12/21 例远处复发事件和 14/17 例死亡。达到 pCR 的患者 DRFS 显著提高(HR=0.23,p=0.009)。
在 H 和 CT 中加入新辅助治疗的 P 是安全的。除腹泻外,两组不良事件发生率 > 2 级无差异。当与 H+CT 联合使用时,P 并未增加心脏毒性,但在我们的人群中,所有心脏事件均发生在接受含蒽环类药物方案的患者中。尽管无统计学意义,但接受新辅助 P+H+CT 的患者可实现更高的 pCR 率。该研究未显示 P 的添加与长期结局之间存在统计学相关性。