Department of Neurosciences, Institute of Human Anatomy, University of Padova, Via Aristide Gabelli 65, 35127 Padova, Italy.
Plastic and Reconstructive Surgery Unit, University of Padova, Via Nicolò Giustiniani 2, 35128 Padova, Italy.
Int J Mol Sci. 2024 Jun 22;25(13):6865. doi: 10.3390/ijms25136865.
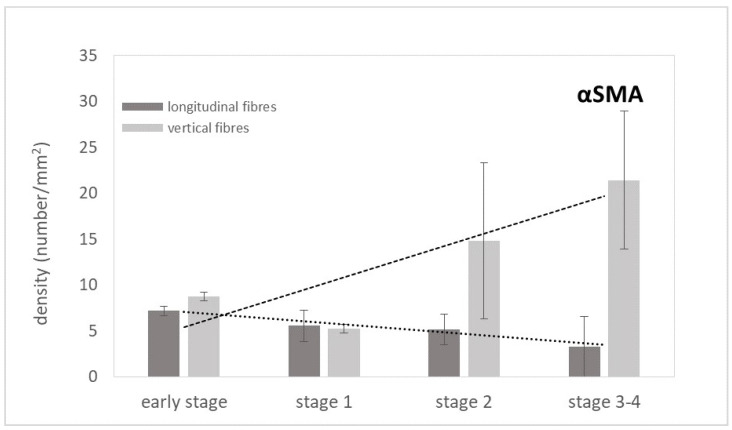
Dupuytren's disease, a chronic and progressive fibroproliferative lesion of the hand, which affects the palmar fascia, has a recurrence rate after selective aponeurotomy of 20-40% at 5 years. This study focused, for the first time, on the microanatomical and histopathological characteristics of the longitudinal and vertical fibres (usually spared during surgery) in the aponeurosis with Dupuytren's disease, in different stages of the Tubiana's classification. Twelve human samples were collected and analysed by immunostaining, Total Collagen Assay, ELISA Immunoassay, and immunoblotting for the Von Willebrand factor, α-Sma, D2-40, CD-68, Total Collagen, Collagen-I and III, IL1β, TNF-α to analyse the blood and lymphatic vascularization, the amount and distribution of collagen, and the inflammation. The results show a progressive increase in the arterial vascularization in the vertical fibres (from 8.8/mm in the early stage to 21.4/mm in stage 3/4), and a parallel progressive decrease in the lymphatic drainage (from 6.2/mm to 2.8/mm), correlated with a local inflammatory context (increase in IL-1β and TNF-α until the stage 2) in both the longitudinal and vertical fibres. The acute inflammation after stage 2 decreased, in favour of a fibrotic action, with the clear synthesis of new collagen (up to ~83 µg/mg), especially Collagen-I. These results clearly demonstrate the involvement of the septa of Legueu and Juvara in the disease pathology and the modifications with the disease's progression. A greater understanding of the pathology becomes fundamental for staging and the adequate therapeutic timing, to obtain the best morpho-functional result and the lowest risk of complications.
掌腱膜挛缩症是一种手部的慢性、进行性纤维增生性病变,影响掌筋膜,选择性切开术后 5 年的复发率为 20-40%。这项研究首次聚焦于掌腱膜挛缩症患者的腱膜中纵向和垂直纤维(手术中通常保留)的微观解剖和组织病理学特征,这些纤维处于 Tubiana 分类的不同阶段。收集了 12 个人类样本,并通过免疫染色、总胶原测定、ELISA 免疫测定和 Von Willebrand 因子、α-Sma、D2-40、CD-68、总胶原、胶原-I 和 III、IL1β、TNF-α的免疫印迹进行分析,以分析血管和淋巴管的血液和淋巴血管化、胶原的数量和分布,以及炎症。结果表明,垂直纤维中的动脉血管化呈渐进性增加(从早期的 8.8/mm 增加到 3/4 期的 21.4/mm),而淋巴引流呈平行渐进性下降(从 6.2/mm 下降到 2.8/mm),这与纵向和垂直纤维中的局部炎症环境(IL-1β和 TNF-α增加到 2 期)相关。2 期后急性炎症减少,有利于纤维化作用,新胶原(高达约 83µg/mg),特别是胶原-I 的明显合成。这些结果清楚地表明,Legueu 和 Juvara 隔层参与了疾病的病理学改变,并随着疾病的进展而发生改变。更好地了解病理学对于分期和适当的治疗时机至关重要,以获得最佳的形态功能结果和最低的并发症风险。