Division of Cardiology, Department of Medicine, University of Verona, Piazzale A. Stefani 1, Verona, Italy.
The Smart Sensors Laboratory and Curam, The Lambe Institute for Translational Medicine, Univesity of Galway, Galway, Ireland.
Clin Res Cardiol. 2024 Dec;113(12):1745-1756. doi: 10.1007/s00392-024-02500-8. Epub 2024 Aug 5.
Physiological patterns of coronary artery disease (CAD) have emerged as potential determinants of functional results of percutaneous coronary interventions (PCI) and of vessel-oriented clinical outcomes (VOCE).
In this study, we evaluated the impact of angiography-derived physiological patterns of CAD on post-PCI functional results and long-term clinical outcomes.
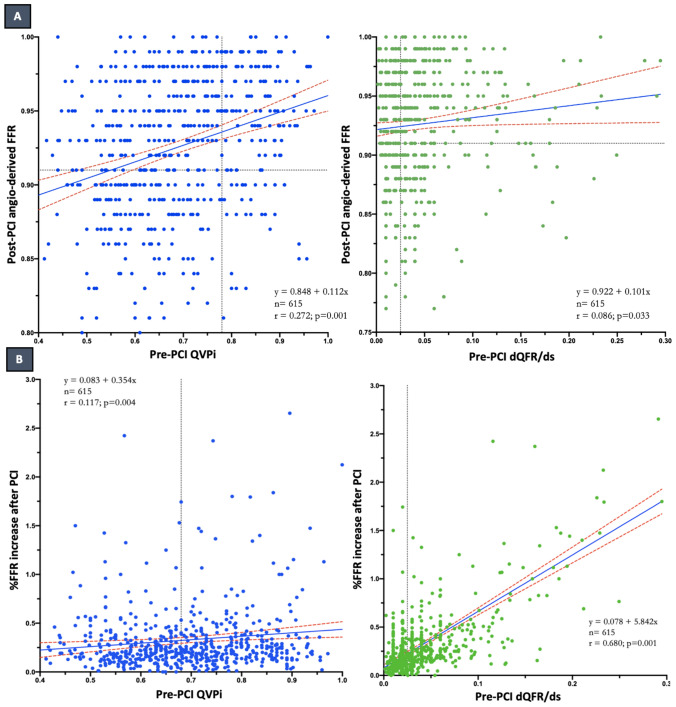
Pre-PCI angiography-derived fractional flow reserve (FFR) virtual pullbacks were quantitatively interpreted and used to determine the physiological patterns of CAD. Suboptimal post-PCI physiology was defined as an angiography-derived FFR value ≤ 0.91. The primary endpoint was the occurrence of VOCE at the longest available follow-up.
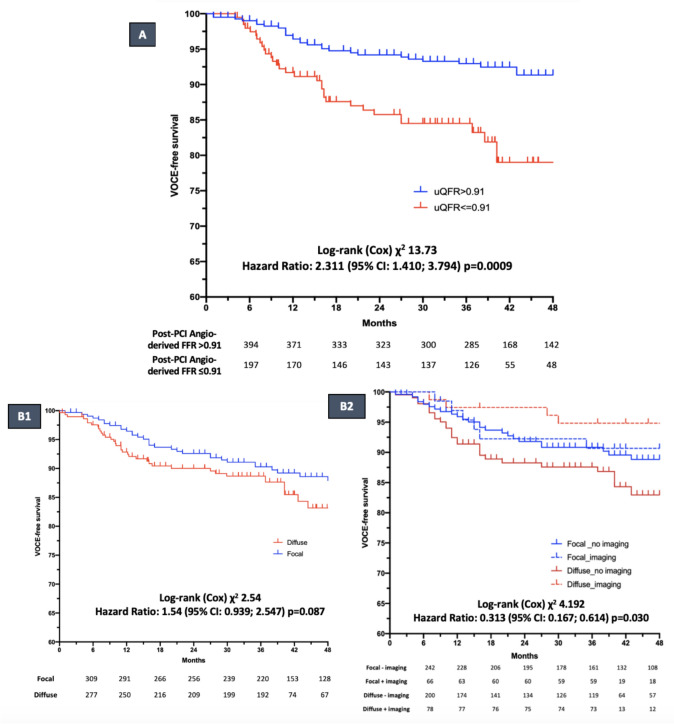
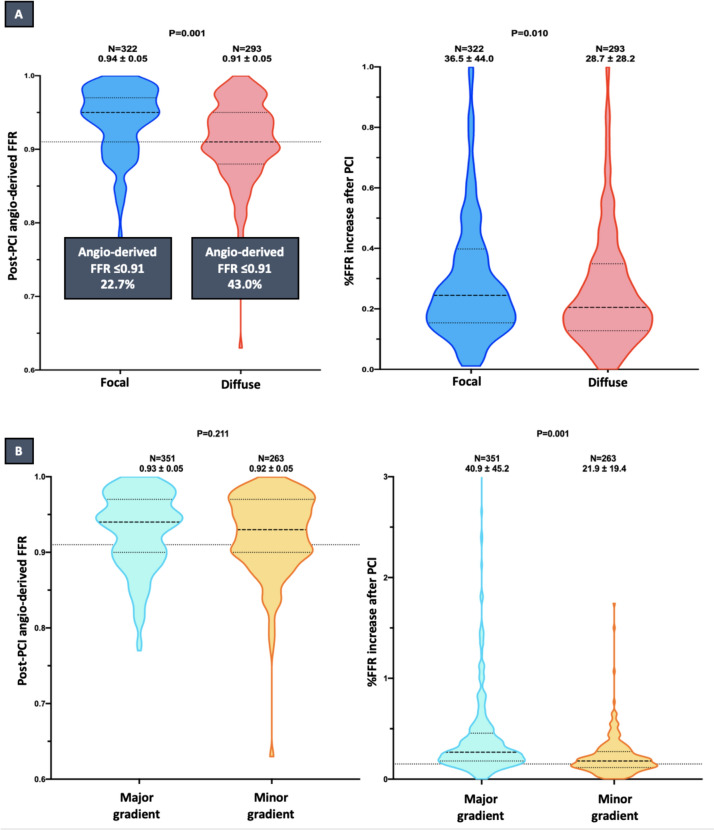
Six hundred fifteen lesions from 516 patients were stratified into predominantly focal (n = 322, 52.3%) and predominantly diffuse (n = 293, 47.7%). Diffuse pattern of CAD was associated with lower post-PCI angiography-derived FFR values (0.91 ± 0.05 vs. 0.94 ± 0.05; p = 0.001) and larger rate of suboptimal post-PCI physiology (43.0 vs. 22.7%; p = 0.001), as compared to focal CAD. At the median follow-up time of 37 months (33-58), post-PCI suboptimal physiology was related to a higher risk of VOCE (16.2% vs. 7.6%; HR: 2.311; 95% CI 1.410-3.794; p = 0.0009), while no significant difference was noted according to baseline physiological pattern. In diffuse disease, the use of intracoronary imaging was associated with a lower incidence of long-term VOCE (5.1% vs 14.8%; HR: 0.313, 95% CI 0.167-0.614, p = 0.030).
Suboptimal post-PCI physiology is observed more often in diffusely diseased arteries and it is associated with higher risk of VOCE at follow-up. The use of intravascular imaging might improve clinical outcomes in the setting of diffuse CAD.
冠心病(CAD)的生理模式已成为经皮冠状动脉介入治疗(PCI)功能结果和血管导向临床结局(VOCE)的潜在决定因素。
本研究旨在评估冠状动脉造影生理模式对 PCI 后功能结果和长期临床结局的影响。
对术前冠状动脉造影衍生的血流储备分数(FFR)虚拟回撤进行定量解读,并用于确定 CAD 的生理模式。定义术后血管造影 FFR 值≤0.91 为术后亚最佳生理状态。主要终点是在最长可随访时间发生 VOCE。
516 例患者的 615 处病变分为主要局灶性(n=322,52.3%)和主要弥漫性病变(n=293,47.7%)。CAD 弥漫性病变与术后血管造影衍生 FFR 值较低(0.91±0.05 比 0.94±0.05;p=0.001)和术后亚最佳生理状态比例较大(43.0%比 22.7%;p=0.001)相关。在 37 个月(33-58 个月)的中位随访时间内,PCI 术后亚最佳生理状态与 VOCE 风险较高相关(16.2%比 7.6%;HR:2.311;95%CI 1.410-3.794;p=0.0009),但与基线生理模式无关。在弥漫性病变中,使用冠状动脉内影像学与长期 VOCE 发生率降低相关(5.1%比 14.8%;HR:0.313,95%CI 0.167-0.614,p=0.030)。
弥漫性病变的动脉中更常观察到 PCI 术后亚最佳生理状态,且与随访时 VOCE 风险增加相关。在弥漫性 CAD 中,使用血管内影像学可能改善临床结局。