Maestre-Luque Luis Carlos, Gonzalez-Manzanares Rafael, Suárez de Lezo Javier, Hidalgo Francisco, Barreiro-Mesa Lucas, de Juan Jaime, Gallo Ignacio, Perea Jorge, Alvarado Marco, Romero Miguel, Ojeda Soledad, Pan Manuel
Department of Cardiology, Reina Sofia University Hospital, Cordoba, Spain.
Maimonides Biomedical Research Institute of Cordoba (IMIBIC), Cordoba, Spain.
Front Cardiovasc Med. 2024 Jul 23;11:1443258. doi: 10.3389/fcvm.2024.1443258. eCollection 2024.
There is current controversy surrounding the benefits of percutaneous coronary intervention (PCI) of chronic total coronary occlusions (CTO). We aimed to evaluate the impact of complete percutaneous revascularization on major adverse cardiovascular events (MACE) in patients with CTO.
A retrospective observational study was conducted of consecutive patients referred for invasive coronary angiography at a single center between January 2018 and December 2019 and at least a CTO. The patients were divided into two groups according to the result of the procedure: complete revascularization of CTO (CR-CTO) versus incomplete revascularization (ICR-CTO) (patients with at least one non-recanalized CTO). Short- and mid-term clinical outcomes were evaluated. The primary endpoint was a composite of MACE that included all-cause death, non-fatal myocardial infarction, non-fatal stroke, or unplanned revascularization.
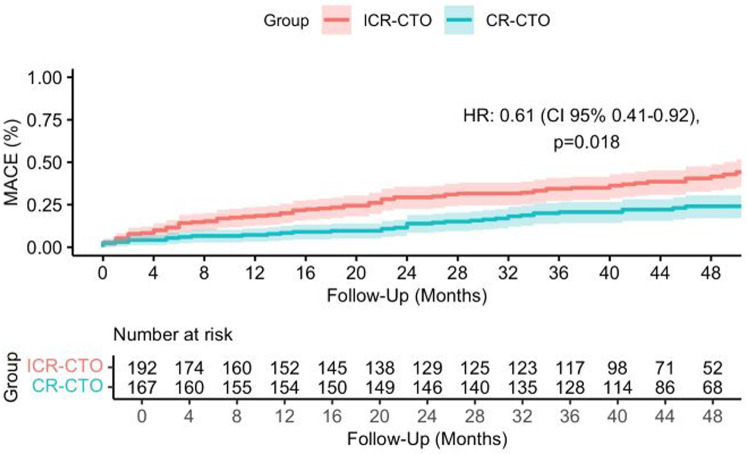
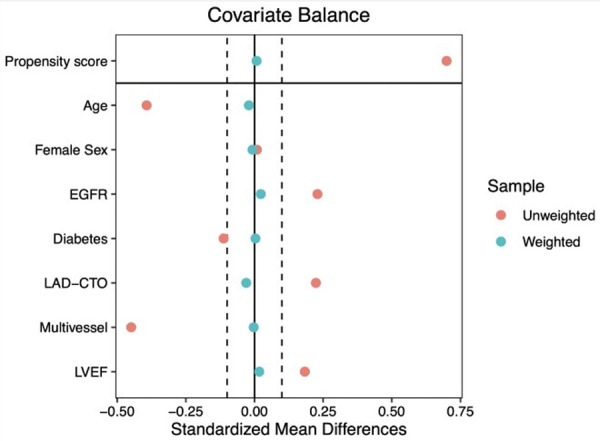
In total, 359 patients with CTO were included. The median age was 68 years [interquartile range (IQR) 60-77 years], 66 (18%) were women and 169 (47.3%) had diabetes mellitus. In all, 167 (46.5%) patients received complete revascularization. After a median follow-up of 42 months (IQR 46-50 months), the primary endpoint occurred in 39 (23.4%) patients in the CR-CTO group and in 75 (39.1%) in the ICR-CTO group (HR 0.50, 95% CI 0.34-0.74; < 0.001). This association remained significant in an inverse probability weighted model considering prognostic factors (adjusted HR 0.61, 95% CI 0.41-0.92; = 0.018) and was driven by lower rates of all-cause death (adjusted OR 0.50, 95% CI 0.23-0.84; = 0.01).
Complete revascularization of CTO was associated with a lower risk of MACE in the midterm follow up.
目前围绕慢性冠状动脉完全闭塞(CTO)的经皮冠状动脉介入治疗(PCI)的益处存在争议。我们旨在评估完全经皮血运重建对CTO患者主要不良心血管事件(MACE)的影响。
对2018年1月至2019年12月期间在单一中心连续接受有创冠状动脉造影且至少有一处CTO的患者进行回顾性观察研究。根据手术结果将患者分为两组:CTO完全血运重建(CR-CTO)组与不完全血运重建(ICR-CTO)组(至少有一处CTO未再通的患者)。评估短期和中期临床结局。主要终点是MACE的复合终点,包括全因死亡、非致命性心肌梗死、非致命性卒中或计划外血运重建。
总共纳入了359例CTO患者。中位年龄为68岁[四分位间距(IQR)60 - 77岁],66例(18%)为女性,169例(47.3%)患有糖尿病。总共167例(46.5%)患者接受了完全血运重建。在中位随访42个月(IQR 46 - 50个月)后,CR-CTO组有39例(23.4%)患者发生主要终点事件,ICR-CTO组有75例(39.1%)患者发生(风险比0.50,95%置信区间0.34 - 0.74;P < 0.001)。在考虑预后因素的逆概率加权模型中,这种关联仍然显著(校正后风险比0.61,95%置信区间0.41 - 0.92;P = 0.018),并且是由全因死亡率较低驱动的(校正后比值比0.50,95%置信区间0.23 - 0.84;P = 0.01)。
CTO完全血运重建与中期随访中较低的MACE风险相关。