Spoormans Eva M, Lemkes Jorrit S, Janssens Gladys N, van der Hoeven Nina W, Jewbali Lucia S D, Dubois Eric A, Meuwissen Martijn, Rijpstra Tom A, Bosker Hans A, Blans Michiel J, Bleeker Gabe B, Baak Remon, Vlachojannis Georgios J, Eikemans Bob J W, van der Harst Pim, van der Horst Iwan C C, Voskuil Michiel, van der Heijden Joris J, Beishuizen Albertus, Stoel Martin, Camaro Cyril, van der Hoeven Hans, Henriques José P, Vlaar Alexander P J, Vink Maarten A, van den Bogaard Bas, Heestermans Ton A C M, de Ruijter Wouter, Delnoij Thijs S R, Crijns Harry J G M, Oemrawsingh Pranobe V, Gosselink Marcel T M, Plomp Koos, Magro Michael, Elbers Paul W G, van der Pas Stéphanie, van Royen Niels
Department of Cardiology, Amsterdam University Medical Center, location VUmc, Amsterdam, the Netherlands.
Department of Cardiology, Erasmus Medical Center, Rotterdam, the Netherlands.
J Soc Cardiovasc Angiogr Interv. 2023 Oct 14;3(2):101191. doi: 10.1016/j.jscai.2023.101191. eCollection 2024 Feb.
In out-of-hospital cardiac arrest (OHCA) without ST-elevation, predictive markers that can identify those with a high risk of acute coronary syndrome are lacking.
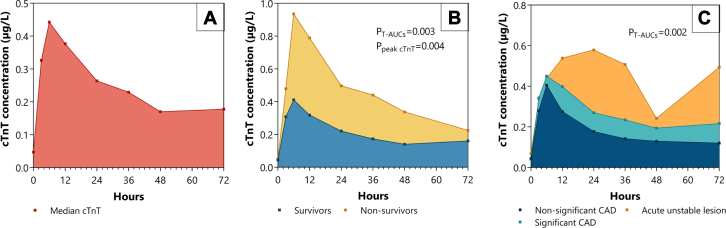
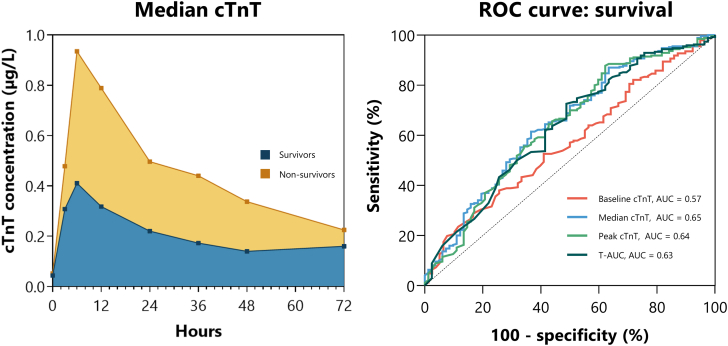
In this post hoc analysis of the Coronary Angiography after Cardiac Arrest (COACT) trial, the baseline, median, peak, and time-concentration curves of troponin-T (cTnT) (T-AUC) in OHCA patients without ST-elevation were studied. cTnT values were obtained at predefined time points at 0, 3, 6, 12, 24, 36, 28, and 72 hours after admission. All patients who died within the measurement period were not included. The primary outcome was the association between cTnT and 90-day survival. Secondary outcomes included the association of cTnT and acute thrombotic occlusions, acute unstable lesions, and left ventricular function.
In total, 352 patients were included in the analysis. The mean age was 64 ± 13 years (80.4% men). All cTnT measures were independent prognostic factors for mortality after adjustment for potential confounders age, sex, history of coronary artery disease, witnessed arrest, time to BLS, and time to return of spontaneous circulation (eg, for T-AUC: hazard ratio, 1.44; 95% CI, 1.06-1.94; = .02; value for all variables ≤.02). Median cTnT (odds ratio [OR], 1.58; 95% CI, 1.18-2.12; = .002) and T-AUC (OR, 2.03; 95% CI, 1.25-3.29; = .004) were independent predictors for acute unstable lesions. Median cTnT (OR, 1.62; 95% CI, 1.17-2.23; = .003) and T-AUC (OR, 2.16; 95% CI, 1.27-3.68; = .004) were independent predictors for acute thrombotic occlusions. CTnT values were not associated with the left ventricular function (eg, for T-AUC: OR, 2.01; 95% CI, 0.65-6.19; = .22; value for all variables ≥.14).
In OHCA patients without ST-segment elevation, cTnT release during the first 72 hours after return of spontaneous circulation was associated with clinical outcomes.
在无ST段抬高的院外心脏骤停(OHCA)中,缺乏能够识别急性冠状动脉综合征高风险患者的预测标志物。
在心脏骤停后冠状动脉造影(COACT)试验的这项事后分析中,研究了无ST段抬高的OHCA患者肌钙蛋白T(cTnT)的基线、中位数、峰值和时间 - 浓度曲线(T - AUC)。在入院后0、3、6、12、24、36、48和72小时的预定义时间点获取cTnT值。测量期内死亡的所有患者均未纳入。主要结局是cTnT与90天生存率之间的关联。次要结局包括cTnT与急性血栓闭塞、急性不稳定病变和左心室功能的关联。
总共352例患者纳入分析。平均年龄为64±13岁(男性占80.4%)。在对潜在混杂因素年龄、性别、冠状动脉疾病史、目击心脏骤停、基础生命支持时间和自主循环恢复时间进行调整后,所有cTnT测量值都是死亡率的独立预后因素(例如,对于T - AUC:风险比,1.44;95%CI,1.06 - 1.94;P = 0.02;所有变量的P值≤0.02)。cTnT中位数(比值比[OR],1.58;95%CI,1.18 - 2.12;P = 0.002)和T - AUC(OR,2.03;95%CI,1.25 - 3.29;P = 0.004)是急性不稳定病变的独立预测因素。cTnT中位数(OR,1.62;95%CI,1.17 - 2.23;P = 0.003)和T - AUC(OR,2.16;95%CI,1.27 - 3.68;P = 0.004)是急性血栓闭塞的独立预测因素。cTnT值与左心室功能无关(例如,对于T - AUC:OR,2.01;95%CI,0.65 - 6.19;P = 0.22;所有变量的P值≥0.14)。
在无ST段抬高的OHCA患者中,自主循环恢复后最初72小时内cTnT的释放与临床结局相关。