Department of Emergency Medicine, Hokkaido University Hospital, N14W5 Kita-Ku, Sapporo, 060-8648, Japan.
Ono Biostat Consulting, Naritahigashi, Suginami-Ku, Tokyo, 166-0015, Japan.
Sci Rep. 2024 Aug 13;14(1):18745. doi: 10.1038/s41598-024-69815-4.
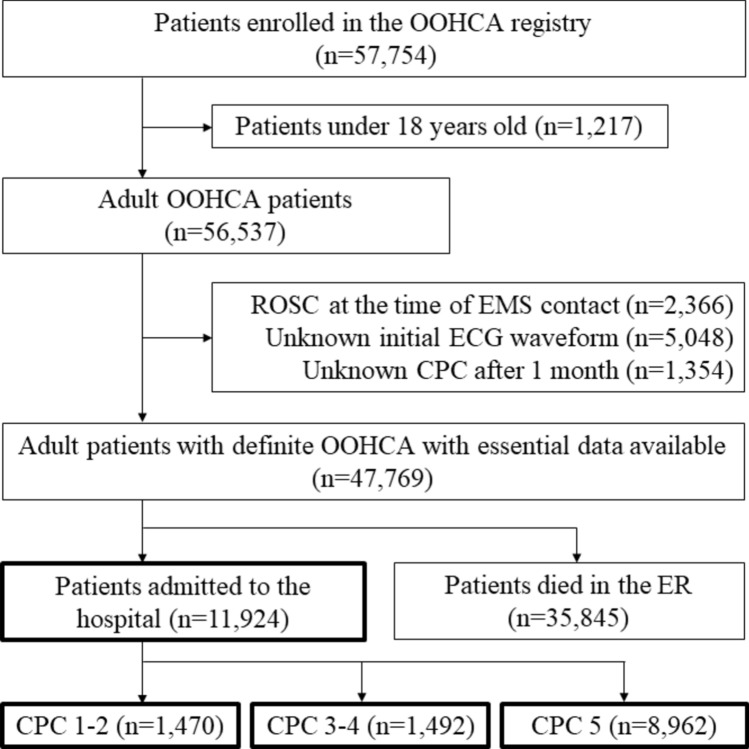
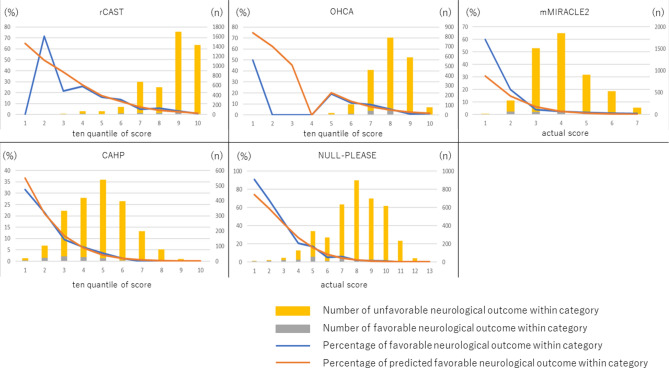
Using a nationwide multicenter prospective registry in Japan's data, we calculated prognostic and predictive scores, including the Out-of-Hospital Cardiac Arrest (OHCA); Cardiac Arrest Hospital Prognosis (CAHP); Nonshockable rhythm, Unwitnessed arrest, Long no-flow or Long low-flow period, blood PH < 7.2, Lactate > 7.0 mmol/L, End-stage chronic kidney disease on dialysis, Age ≥ 85 years, Still resuscitation, and Extracardiac cause (NULL-PLEASE); revised post-Cardiac Arrest Syndrome for Therapeutic hypothermia (rCAST); and MIRACLE2 scores, for adult patients with cardiac arrest. The MIRACLE2 score was validated with the modified MIRACLE2 score, which excludes information of pupillary reflexes. Each score was calculated only for the cases with no missing data for the variables used. These scores' accuracies were compared using neurological outcomes 30 days after out-of-hospital cardiac arrest (OOHCA). Patients with a cerebral performance category scale of 1 or 2 were designated as having favorable neurological outcomes. Each score's discrimination ability was evaluated by the receiver operating characteristic curve's area under the curve (AUC). To assess in detail in areas of high specificity and high sensitivity, which are areas of interest to clinicians, partial AUCs were also used. The analysis included 11,924 hospitalized adult patients. The AUCs of the OHCA, MIRACLE2, CAHP, rCAST, and NULL-PLEASE scores for favorable neurological outcomes were 0.713, 0.727, 0.785, 0.761, and 0.831, respectively. The CAHP and NULL-PLEASE scores were significantly more accurate than the rest. Accuracies did not differ significantly between the CAHP and NULL-PLEASE scores. The NULL-PLEASE score was significantly better at discriminating favorable neurological prognoses at 30 days in patients with OOHCA compared to other scoring systems.
利用日本全国多中心前瞻性登记处的数据,我们计算了预后和预测评分,包括院外心脏骤停(OHCA)、心脏骤停医院预后(CAHP)、非电击性节律、无目击骤停、长时间无血流或低血流期、血 pH 值<7.2、乳酸>7.0mmol/L、终末期慢性肾脏病透析、年龄≥85 岁、仍在复苏中、心外原因(NULL-PLEASE);修订后心脏骤停后综合征低温治疗(rCAST)和 MIRACLE2 评分,用于心脏骤停的成年患者。使用排除瞳孔反射信息的改良 MIRACLE2 评分对 MIRACLE2 评分进行了验证。仅对变量无缺失数据的病例计算每个评分。使用 30 天后院外心脏骤停(OOHCA)的神经功能结局比较这些评分的准确性。格拉斯哥预后评分(GOS)为 1 或 2 的患者被指定为神经功能结局良好。通过接收者操作特征曲线下面积(AUC)评估每个评分的区分能力。为了详细评估对临床医生感兴趣的高特异性和高灵敏度区域,还使用了部分 AUC。分析包括 11924 名住院成年患者。OHCA、MIRACLE2、CAHP、rCAST 和 NULL-PLEASE 评分对良好神经功能结局的 AUC 分别为 0.713、0.727、0.785、0.761 和 0.831。CAHP 和 NULL-PLEASE 评分明显更准确。CAHP 和 NULL-PLEASE 评分之间的准确性没有显著差异。与其他评分系统相比,NULL-PLEASE 评分在区分 OOHCA 患者 30 天的良好神经预后方面表现更优。