Akinbobola Olawale, Liao Wei, Ray Meredith A, Fehnel Carrie, Goss Jordan, Qureshi Talat, Saulsberry Andrea, Dortch Kourtney, Smeltzer Matthew P, Osarogiagbon Raymond U
Thoracic Oncology Research Group, Baptist Cancer Center, Memphis, Tennessee.
School of Public Health, University of Memphis, Memphis, Tennessee.
JTO Clin Res Rep. 2024 May 16;5(8):100684. doi: 10.1016/j.jtocrr.2024.100684. eCollection 2024 Aug.
Early lung cancer detection programs improve surgical resection rates and survival but may skew toward more indolent cancers.
Hypothesizing that differences in stage-stratified survival indicate differences in biological aggressiveness and possible length-time and overdiagnosis bias, we assessed a cohort who had curative-intent resection, categorized by diagnostic pathways: screening, incidental pulmonary nodule program, and non-program based. Survival was analyzed using Kaplan-Meier plots, log-rank tests, and Cox regression, comparing aggregate and stage-stratified survival across cohorts with Tukey's method for multiple testing.
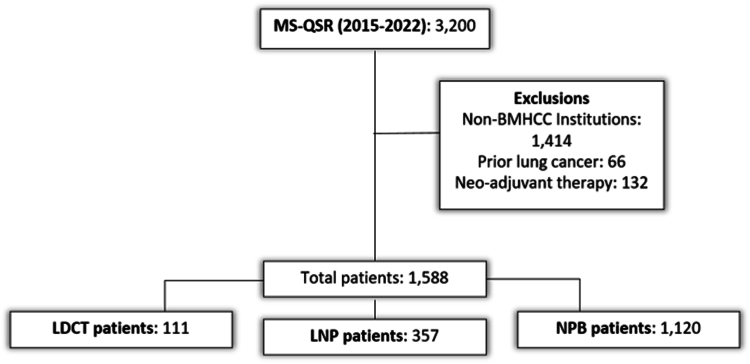
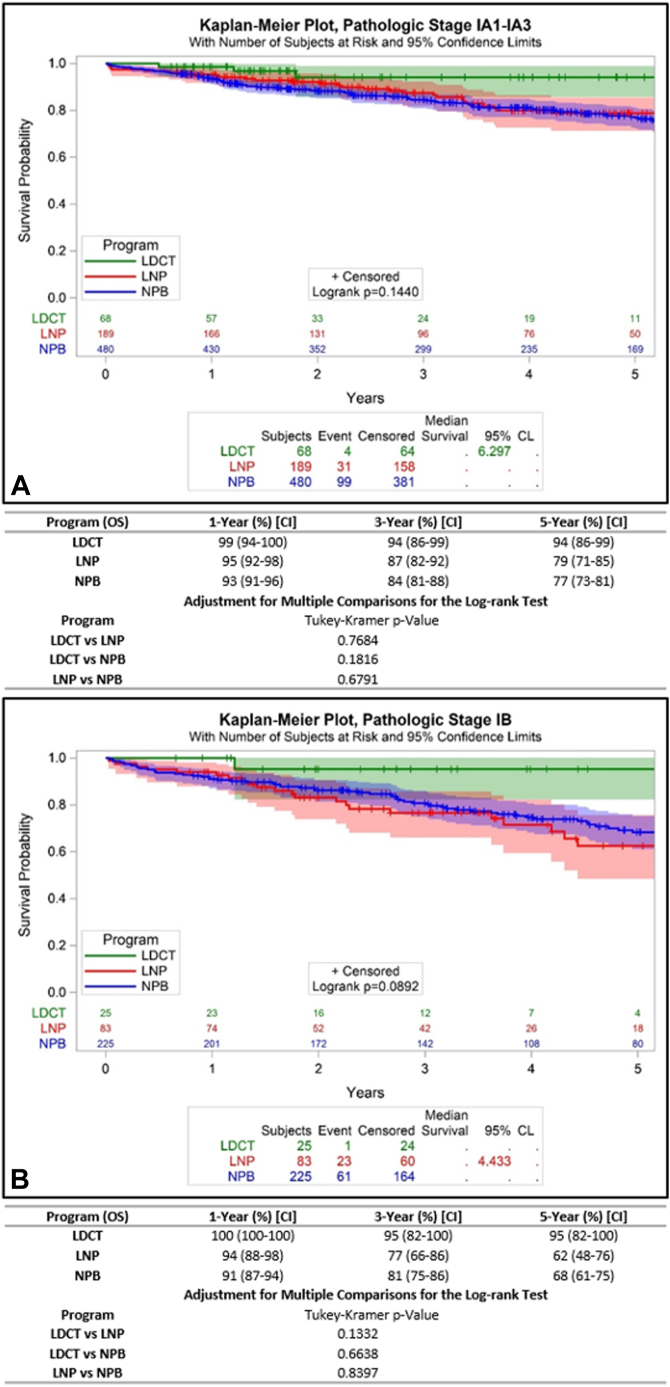
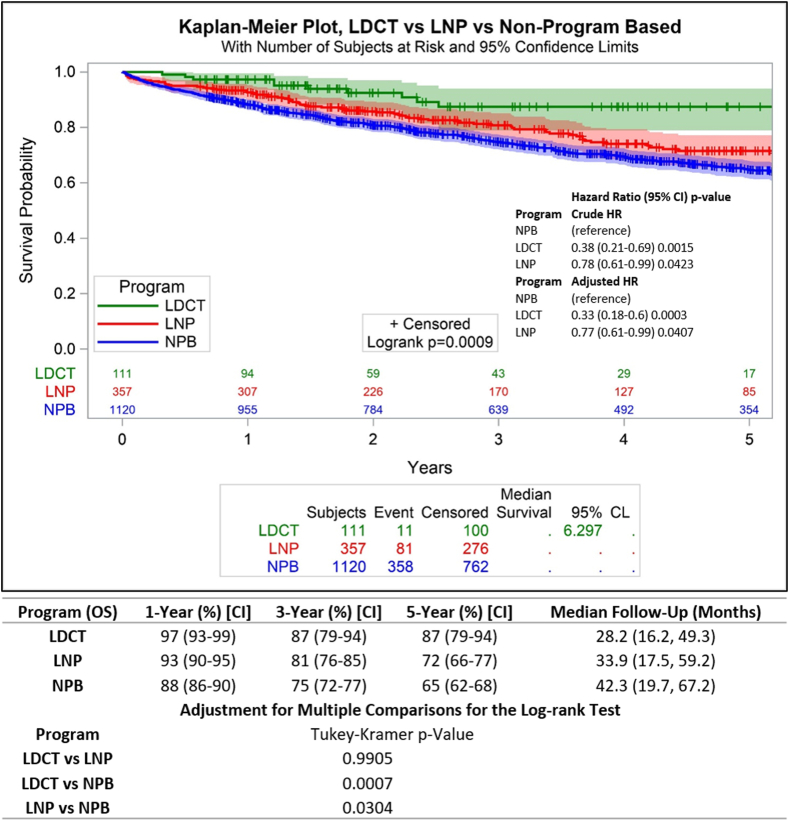
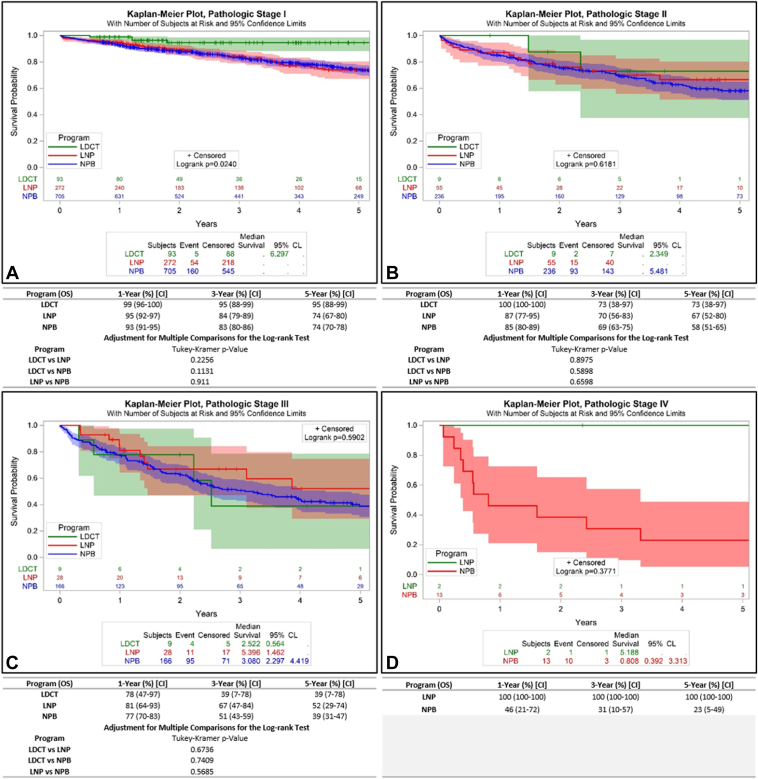
Of 1588 patients, 111 patients (7%), 357 patients (22.5%), and 1120 patients (70.5%) were diagnosed through screening, pulmonary nodule, and non-program-based pathways; 0% versus 9% versus 6% were older than 80 years ( = 0.0048); 17%, 23%, and 24% had a Charlson Comorbidity score greater than or equal to 2 ( = 0.0143); 7%, 6%, and 9% had lepidic adenocarcinoma; 26%, 31%, and 34% had poorly or undifferentiated tumors ( = 0.1544); and 93%, 87%, and 77% had clinical stage I ( < 0.0001).Aggregate 5-year survival was 87%, 72%, and 65% ( = 0.0009), including 95%, 74%, and 74% for pathologic stage I. Adjusted pairwise comparisons showed similar survival in screening and nodule program cohorts ( = 0.9905). Nevertheless, differences were significant between screening and non-program-based cohorts ( = 0.0007, adjusted hazard ratio 0.33 [95% confidence interval: 0.18-0.6]) and between nodule and nonprogram cohorts (adjusted hazard ratio 0.77 [95% confidence interval: 0.61-0.99]). Stage I comparisons yielded = 0.2256, 0.1131, and 0.911. In respective pathways, 0%, 2%, and 2% of patients with stage I disease who were older than 80 years had a Charlson score greater than or equal to 2 ( = 0.3849).
Neither length-time nor overdiagnosis bias was evident in NSCLC diagnosed through screening or incidental pulmonary nodule programs.
早期肺癌检测项目可提高手术切除率和生存率,但可能偏向于更多惰性癌症。
假设按分期分层的生存率差异表明生物学侵袭性、可能的时长和过度诊断偏倚存在差异,我们评估了一组接受根治性切除的患者,根据诊断途径进行分类:筛查、偶然肺结节项目和非项目途径。使用Kaplan-Meier曲线、对数秩检验和Cox回归分析生存率,采用Tukey多重检验方法比较各队列的总体生存率和分期分层生存率。
在1588例患者中,111例(7%)、357例(22.5%)和1120例(70.5%)分别通过筛查、肺结节和非项目途径诊断;80岁以上患者比例分别为0%、9%和6%(P = 0.0048);Charlson合并症评分大于或等于2的患者分别为17%、23%和24%(P = 0.0143);鳞屑样腺癌患者分别为7%、6%和9%;低分化或未分化肿瘤患者分别为26%、31%和34%(P = 0.1544);临床I期患者分别为93%、87%和77%(P < 0.0001)。总体5年生存率分别为87%、72%和65%(P = 0.0009),病理I期患者分别为95%、74%和74%。调整后的两两比较显示筛查队列和肺结节项目队列的生存率相似(P = 0.9905)。然而,筛查队列和非项目队列之间存在显著差异(P = 0.0007,调整后风险比0.33 [95%置信区间:0.18 - 0.6]),肺结节队列和非项目队列之间也存在显著差异(调整后风险比0.77 [95%置信区间:0.61 - 0.99])。I期比较的P值分别为0.2256、0.1131和0.911。在各途径中,80岁以上I期疾病患者中Charlson评分大于或等于2的患者分别为0%、2%和2%(P = 0.3849)。
通过筛查或偶然肺结节项目诊断的非小细胞肺癌中,未发现时长或过度诊断偏倚。