Department of Ophthalmology and Visual Sciences, Heersink School of Medicine, University of Alabama at Birmingham, Birmingham, Alabama, United States.
Department of Ophthalmology, University of Bonn, Bonn, Germany.
Invest Ophthalmol Vis Sci. 2024 Aug 1;65(10):25. doi: 10.1167/iovs.65.10.25.
In AMD, rod-mediated dark adaptation (RMDA) at 5° eccentricity is slower in eyes with subretinal drusenoid deposits (SDDs) than in eyes without. Here we quantified SDD burden using supervised deep learning for comparison to vision and photoreceptor topography.
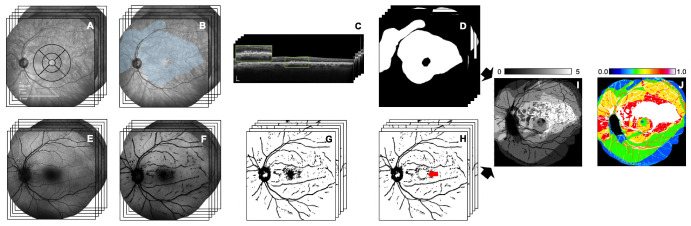
In persons ≥60 years from the Alabama Study on Early Age-Related Macular Degeneration 2, normal, early AMD, and intermediate AMD eyes were classified by the AREDS nine-step system. A convolutional neural network was trained on 55°-wide near-infrared reflectance images for SDD segmentation. Trained graders annotated ground truth (SDD yes/no). Predicted and true datasets agreed (Dice coefficient, 0.92). Inference was manually proofread using optical coherence tomography. The mean SDD area (mm2) was compared among diagnostic groups (linear regression) and to vision (age-adjusted Spearman correlations). Fundus autofluorescence images were used to mask large vessels in SDD maps.
In 428 eyes of 428 persons (normal, 218; early AMD, 120; intermediate AMD, 90), the mean SDD area differed by AMD severity (P < 0.0001): 0.16 ± 0.87 (normal), 2.48 ± 11.23 (early AMD), 11.97 ± 13.33 (intermediate AMD). Greater SDD area was associated with worse RMDA (r = 0.27; P < 0.0001), mesopic (r = -0.13; P = 0.02) and scotopic sensitivity (r = -0.17; P < 0.001). SDD topography peaked at 5° superior, extended beyond the Early Treatment of Diabetic Retinopathy Study grid and optic nerve, then decreased.
SDD area is associated with degraded rod-mediated vision. RMDA 5° (superior retina) probes where SDD is maximal, closer to the foveal center than the rod peak at 3 to 6 mm (10.4°-20.8°) superior and the further eccentric peak of rod:cone ratio. Topographic data imply that factors in addition to rod density influence SDD formation.
在 AMD 中,5°偏心度的杆状介导暗适应(RMDA)在有视网膜下类脂沉积(SDD)的眼睛中比在没有 SDD 的眼睛中慢。在这里,我们使用监督深度学习来定量 SDD 负担,并与视力和光感受器地形图进行比较。
在来自阿拉巴马州早期年龄相关性黄斑变性 2 研究的年龄≥60 岁的人群中,正常、早期 AMD 和中间 AMD 眼按 AREDS 九步系统进行分类。在 55°宽近红外反射图像上训练卷积神经网络进行 SDD 分割。训练有素的分级员对地面实况(SDD 是/否)进行注释。预测数据集和真实数据集一致(Dice 系数,0.92)。推理使用光学相干断层扫描手动校对。在诊断组之间比较平均 SDD 面积(mm2)(线性回归)和视力(年龄调整 Spearman 相关)。使用眼底自发荧光图像在 SDD 图中掩蔽大血管。
在 428 名 428 名患者(正常 218 名,早期 AMD 120 名,中间 AMD 90 名)的 428 只眼中,SDD 面积因 AMD 严重程度而异(P <0.0001):0.16 ± 0.87(正常),2.48 ± 11.23(早期 AMD),11.97 ± 13.33(中间 AMD)。较大的 SDD 面积与较差的 RMDA 相关(r = 0.27;P <0.0001)、中值(r = -0.13;P = 0.02)和暗视力(r = -0.17;P <0.001)。SDD 地形图在 5°上方达到峰值,延伸超出早期糖尿病视网膜病变研究网格和视神经,然后下降。
SDD 面积与杆状介导视力下降有关。RMDA 5°(上视网膜)探测 SDD 最大的位置,比 3 至 6 毫米(10.4°-20.8°)上方的杆状峰和更远的偏心杆:锥比峰更接近中央凹中心。地形数据表明,除了杆密度之外,还有其他因素影响 SDD 的形成。