Nomoto Mikako, Kidani Tomoki, Kida Masayoshi, Kobayashi Koji, Fujimi Yosuke, Kawamoto Saki, Izutsu Nobuyuki, Asai Katsunori, Kanemura Yonehiro, Nakajima Shin, Fujinaka Toshiyuki
Department of Neurosurgery, NHO Osaka National Hospital, Osaka, Osaka, Japan.
J Neuroendovasc Ther. 2024;18(8):219-223. doi: 10.5797/jnet.oa.2024-0038. Epub 2024 Jul 4.
Treatment of anterior choroidal artery (AChA) aneurysms is frequently associated with ischemic complications. This study aimed to report the outcomes of treatment of unruptured AChA aneurysms in our hospital.
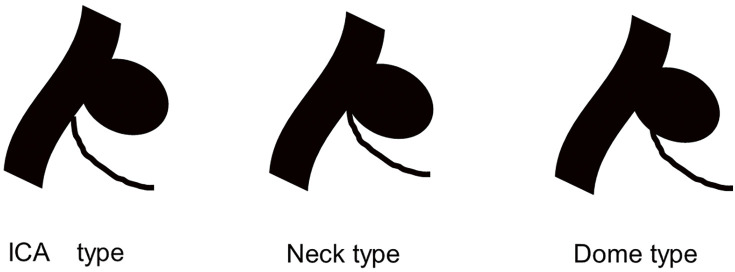
Between January 2015 and March 2022, 40 patients were treated for an unruptured AChA aneurysm in our hospital. Age, sex, aneurysm size, AChA branching type, treatment, occlusion rate, complications, modified Rankin Scale (mRS) score before surgery and after 90 days, and recurrence were investigated. The branching type was classified as internal carotid artery (ICA), neck, or dome type based on the location of the AChA origin.
The mean age was 61.1 ± 1.9 years; 15 patients were men and 25 were women. The mean aneurysm diameter was 4.4 ± 0.3 mm. The branching type was ICA in four patients, neck in 35, and dome in one. Treatment was surgical clipping in 22 patients and endovascular coil embolization in 18 (14 with stent assistance). Motor-evoked potential (MEP) monitoring was used in all patients of the clipping group and 9 cases of the coiling group. Treatment complications occurred in eight patients (20%). mRS score worsened by more than one point 90 days after treatment in four patients (10%); however, the proportion of patients who experienced this did not significantly differ between the clipping and coiling groups. Although the odds of a thrombotic complication were higher with coiling than clipping, the difference was not significant (odds ratio: 10.2; P = 0.08). The rate of complete occlusion was lower in the coiling group (72.2% vs. 95.3%), but the difference was not significant. The median follow-up was 696 days (range: 99-2053). No aneurysm recurrence or rupture occurred.
AChA branching type is important for treatment decision-making in patients with AChA aneurysms. Rates of complications and occlusion do not significantly differ between clipping and coiling of AChA aneurysms. MEP monitoring may be useful in preventing thrombotic complications during coil embolization.
脉络膜前动脉(AChA)动脉瘤的治疗常伴有缺血性并发症。本研究旨在报告我院未破裂AChA动脉瘤的治疗结果。
2015年1月至2022年3月期间,我院对40例未破裂AChA动脉瘤患者进行了治疗。调查了患者的年龄、性别、动脉瘤大小、AChA分支类型、治疗方式、闭塞率、并发症、术前及90天后的改良Rankin量表(mRS)评分以及复发情况。根据AChA起源部位,将分支类型分为颈内动脉(ICA)型、颈部型或瘤顶型。
患者平均年龄为61.1±1.9岁;男性15例,女性25例。动脉瘤平均直径为4.4±0.3mm。分支类型为ICA型4例,颈部型35例,瘤顶型1例。22例患者接受了手术夹闭治疗,18例(其中14例有支架辅助)接受了血管内弹簧圈栓塞治疗。夹闭组所有患者及弹簧圈栓塞组9例患者使用了运动诱发电位(MEP)监测。8例患者(20%)出现治疗并发症。4例患者(10%)在治疗90天后mRS评分恶化超过1分;然而,夹闭组和弹簧圈栓塞组出现这种情况的患者比例无显著差异。虽然弹簧圈栓塞治疗血栓形成并发症的几率高于夹闭治疗,但差异不显著(优势比:10.2;P=0.08)。弹簧圈栓塞组的完全闭塞率较低(72.2%对95.3%),但差异不显著。中位随访时间为696天(范围:99-2053天)。未发生动脉瘤复发或破裂。
AChA分支类型对AChA动脉瘤患者的治疗决策很重要。AChA动脉瘤夹闭和弹簧圈栓塞治疗的并发症发生率和闭塞率无显著差异。MEP监测可能有助于预防弹簧圈栓塞过程中的血栓形成并发症。