Honaryar M K, Locquet M, Allodji R, Jimenez G, Pinel B, Lairez O, Panh L, Camilleri J, Broggio D, Ferrières J, De Vathaire F, Jacob S
CESP, Radiation Epidemiology Team, INSERM U 1018, Villejuif, 94800, France.
Research Department, Gustave Roussy, Villejuif, 94800, France.
Cardiooncology. 2024 Aug 26;10(1):54. doi: 10.1186/s40959-024-00255-9.
Radiation therapy (RT) for breast cancer (BC) can result in subtle cardiac dysfunction that can occur early after treatment. In 2022, the European Society of Cardiology (ESC) published the first guidelines in cardio-oncology with a harmonized definition of cancer therapy-related cardiac dysfunction (CTRCD). The aim of this study was to evaluate CTRCD occurrence over 24 months of follow-up after RT in BC patients and to analyze the association with cardiac radiation exposure.
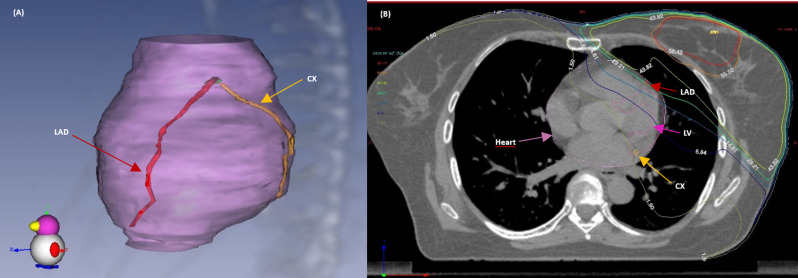
The prospective monocentric BACCARAT study included BC patients treated with RT without chemotherapy, aged 40-75 years, with conventional and 2D Speckle tracking echocardiography performed before RT, 6 and 24 months after RT. Based on ESC cardio-oncology guidelines, CTRCD and corresponding severity were defined with left ventricle ejection fraction and global longitudinal strain decrease, occurring at 6 or 24 months after RT. Dosimetry for whole heart, left ventricle (LV) and left coronary artery (left anterior descending and circumflex arteries (CX)) was considered to evaluate the association with CTRCD, based on logistic regressions (Odds Ratio - OR and 95% confidence interval - 95%CI). Youden index based on receiver operating characteristic curve analysis was used to identify the optimal threshold of dose-volume parameters for predicting CTRCD.
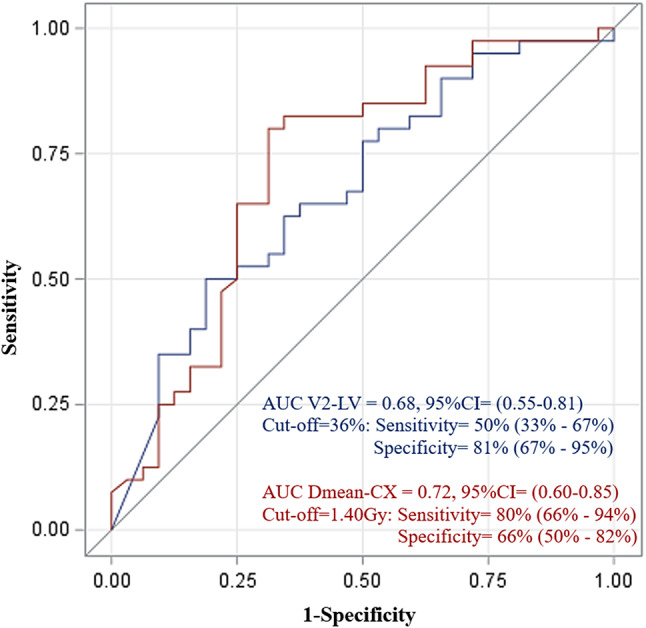
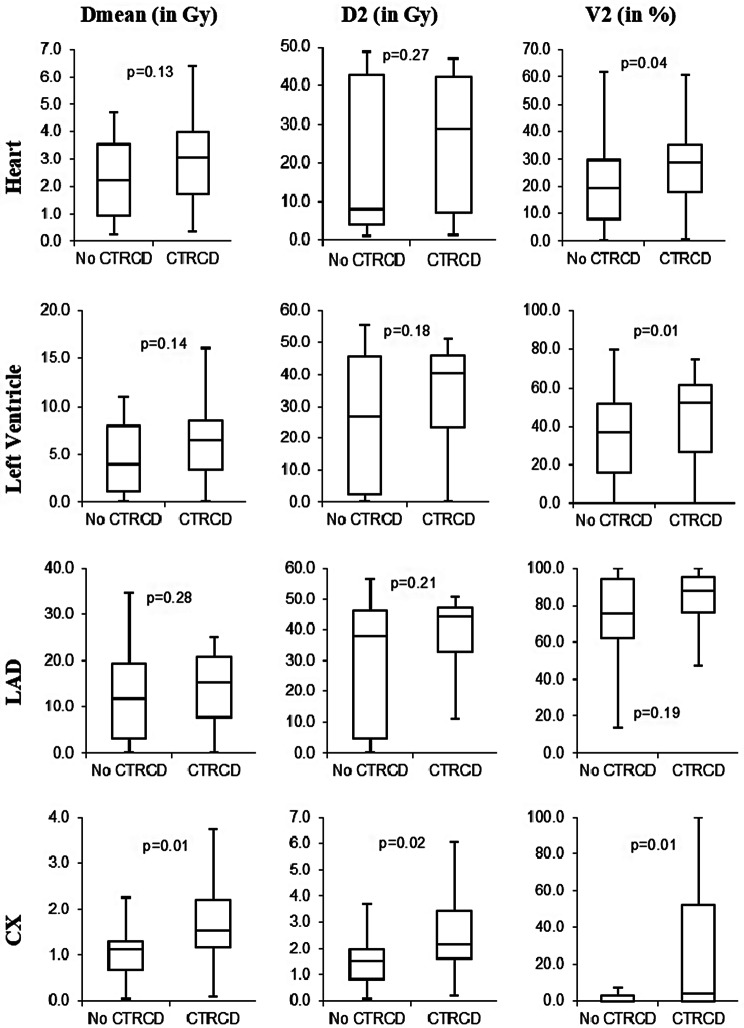
The study included 72 BC patients with a mean age of 58 ± 8.2 years. A total of 32 (44%) patients developed CTRCD during follow-up: 20 (28%) mild CTRCD, 7 (9%) moderate CTRCD, and 5 (7%) severe CTRCD. Cardiac radiation doses were generally higher among patients with CTRCD rather than non-CTRCD. Dose-response relationships were significant for mean CX dose (OR = 2.48, 95%CI (1.12-5.51), p = 0.02) and marginally significant for V2 of LV (OR = 1.03 95%CI (1.00-1.06), p = 0.05). V2 of LV ≥ 36% and mean CX dose ≥ 1.40 Gy thresholds were determined to be optimal for predicting CTRCD.
For BC patients treated with RT without chemotherapy, CTRCD can be observed in an important proportion of the population over 24 months after treatment. Left ventricle and circumflex coronary artery exposure were found to be associated with CTRCD and could be used for the prediction of such cardiotoxicity. Further research remains needed to confirm these results.
ClinicalTrials.gov Identifier- NCT02605512.
乳腺癌(BC)放疗(RT)可导致细微的心脏功能障碍,且可能在治疗后早期出现。2022年,欧洲心脏病学会(ESC)发布了心脏肿瘤学领域的首个指南,对癌症治疗相关心脏功能障碍(CTRCD)给出了统一的定义。本研究的目的是评估BC患者放疗后24个月随访期间CTRCD的发生情况,并分析其与心脏辐射暴露的关联。
前瞻性单中心BACCARAT研究纳入了年龄在40 - 75岁、接受放疗且未接受化疗的BC患者,在放疗前、放疗后6个月和24个月进行常规及二维斑点追踪超声心动图检查。根据ESC心脏肿瘤学指南,依据放疗后6个月或24个月时左心室射血分数和整体纵向应变降低来定义CTRCD及其相应严重程度。基于逻辑回归(优势比 - OR和95%置信区间 - 95%CI),考虑全心脏、左心室(LV)和左冠状动脉(左前降支和回旋支动脉(CX))的剂量测定,以评估其与CTRCD的关联。基于受试者工作特征曲线分析的约登指数用于确定预测CTRCD的剂量 - 体积参数的最佳阈值。
该研究纳入了72例BC患者,平均年龄为58 ± 8.2岁。共有32例(44%)患者在随访期间发生CTRCD:20例(28%)为轻度CTRCD,7例(9%)为中度CTRCD,5例(7%)为重度CTRCD。发生CTRCD的患者心脏辐射剂量总体上高于未发生CTRCD的患者。平均CX剂量的剂量 - 反应关系显著(OR = 2.48,95%CI(1.12 - 5.51),p = 0.02),LV的V2剂量 - 反应关系边缘显著(OR = 1.03,95%CI(1.00 - 1.06),p = 0.05)。LV的V2≥36%和平均CX剂量≥1.40 Gy的阈值被确定为预测CTRCD的最佳阈值。
对于接受放疗且未接受化疗的BC患者,在治疗后24个月内,相当一部分人群可观察到CTRCD。发现左心室和回旋冠状动脉暴露与CTRCD相关,可用于预测此类心脏毒性。仍需进一步研究以证实这些结果。
ClinicalTrials.gov标识符 - NCT02605512。