Passarelli Maria Teresa, Petit Matthieu, Garberi Roberta, Lebreton Guillaume, Luyt Charles Edouard, Pineton De Chambrun Marc, Chommeloux Juliette, Hékimian Guillaume, Rezoagli Emanuele, Foti Giuseppe, Combes Alain, Giani Marco, Schmidt Matthieu
Department of Medicine and Surgery, University of Milano-Bicocca, Monza, Italy.
Department of Emergency and Intensive Care, Fondazione IRCCS San Gerardo Dei Tintori, Monza, Italy.
Ann Intensive Care. 2024 Sep 4;14(1):138. doi: 10.1186/s13613-024-01359-2.
The optimal timing of weaning from venovenous extracorporeal membrane oxygenation (VV ECMO) and its modalities have been rarely studied.
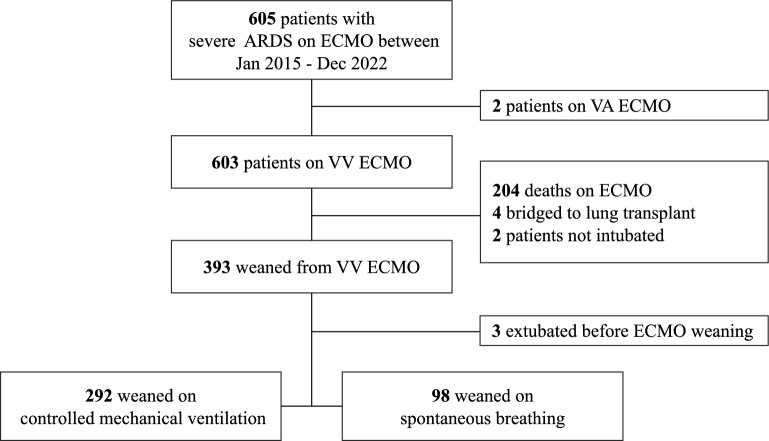
Retrospective, multicenter cohort study over 7 years in two tertiary ICUs, high-volume ECMO centers in France and Italy. Patients with ARDS on ECMO and successfully weaned from VV ECMO were classified based on their mechanical ventilation modality during the sweep gas-off trial (SGOT) with either controlled mechanical ventilation or spontaneous breathing (i.e. pressure support ventilation). The primary endpoint was the time to successful weaning from mechanical ventilation within 90 days post-ECMO weaning.
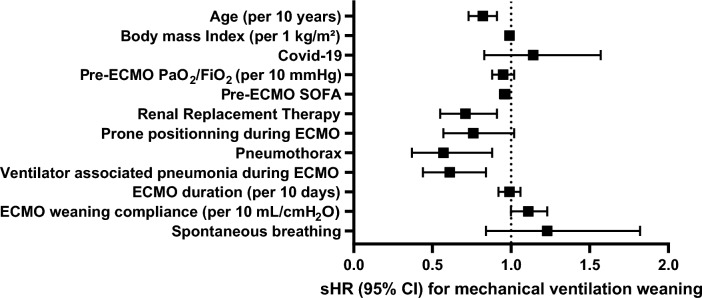
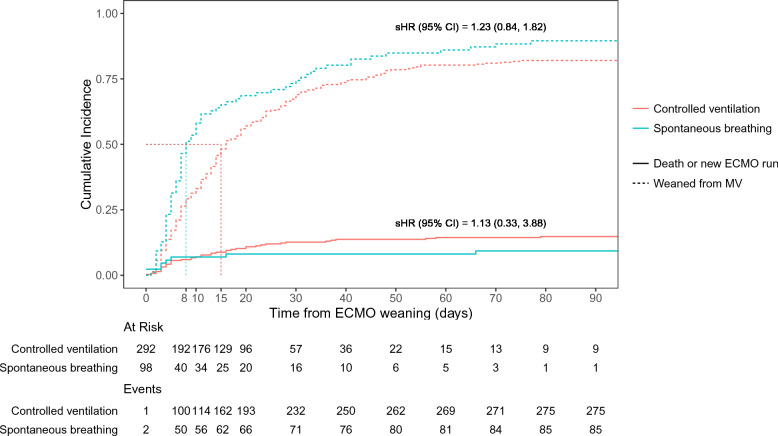
292 adult patients with severe ARDS were weaned from controlled ventilation, and 101 were on spontaneous breathing during SGOT. The 90-day probability of successful weaning from mechanical ventilation was not significantly different between the two groups (sHR [95% CI], 1.23 [0.84-1.82]). ECMO-related complications were not statistically different between patients receiving these two mechanical ventilation strategies. After adjusting for covariates, older age, higher pre-ECMO sequential organ failure assessment score, pneumothorax, ventilator-associated pneumonia, and renal replacement therapy, but not mechanical ventilation modalities during SGOT, were independently associated with a lower probability of successful weaning from mechanical ventilation after ECMO weaning.
Time to successful weaning from mechanical ventilation within 90 days post-ECMO was not associated with the mechanical ventilation strategy used during SGOT. Further research is needed to assess the optimal ventilation strategy during weaning off VV ECMO and its impact on short- and long-term outcomes.
静脉-静脉体外膜肺氧合(VV ECMO)撤机的最佳时机及其方式鲜有研究。
在法国和意大利的两家大型ECMO中心的三级重症监护病房进行了一项为期7年的回顾性多中心队列研究。对接受ECMO治疗且成功从VV ECMO撤机的急性呼吸窘迫综合征(ARDS)患者,根据其在无气体支持试验(SGOT)期间的机械通气方式进行分类,分为控制机械通气或自主呼吸(即压力支持通气)。主要终点是ECMO撤机后90天内成功脱离机械通气的时间。
292例成年重症ARDS患者从控制通气撤机,101例在SGOT期间进行自主呼吸。两组患者90天内成功脱离机械通气的概率无显著差异(sHR [95% CI],1.23 [0.84 - 1.82])。接受这两种机械通气策略的患者ECMO相关并发症在统计学上无差异。在对协变量进行调整后,年龄较大、ECMO前序贯器官衰竭评估评分较高、气胸、呼吸机相关性肺炎和肾脏替代治疗,但不是SGOT期间的机械通气方式,与ECMO撤机后成功脱离机械通气的概率较低独立相关。
ECMO撤机后90天内成功脱离机械通气的时间与SGOT期间使用的机械通气策略无关。需要进一步研究以评估VV ECMO撤机期间的最佳通气策略及其对短期和长期预后的影响。