Schurink Ivo J, de Goeij Femke H C, van der Heijden Fenna J, van Rooden Rutger M, van Dijk Madeleine C, Polak Wojciech G, van der Laan Luc J W, Huurman Volkert A L, de Jonge Jeroen
Division of HPB and Transplant Surgery, Department of Surgery, Erasmus MC Transplant Institute, Erasmus University Medical Center, Doctor Molewaterplein 40, 3015 GD Rotterdam, Zuid Holland The Netherlands.
LUMC Transplant Center, Department of Surgery, Leiden University Medical Center, Leiden, The Netherlands.
EPMA J. 2024 Jul 16;15(3):545-558. doi: 10.1007/s13167-024-00371-7. eCollection 2024 Sep.
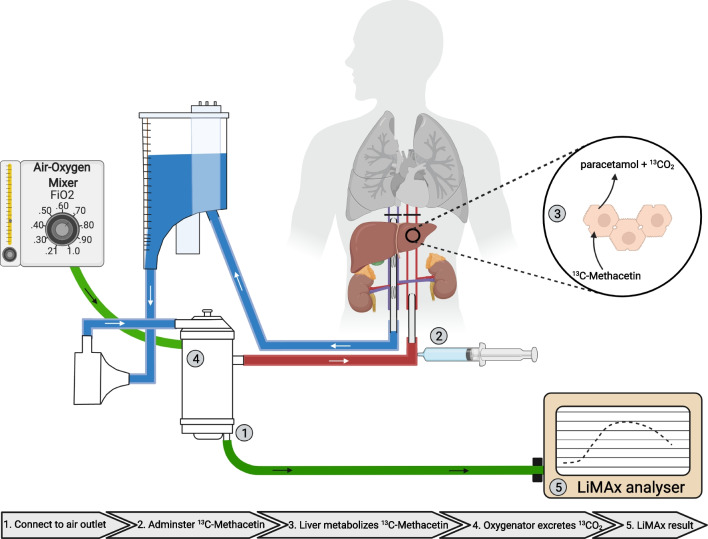
In an effort to reduce waitlist mortality, extended criteria donor organs, including those from donation after circulatory death (DCD), are being used with increasing frequency. These donors carry an increased risk for postoperative complications, and balancing donor-recipient risks is currently based on generalized nomograms. Abdominal normothermic regional perfusion (aNRP) enables individual evaluation of DCD organs, but a gold standard to determine suitability for transplantation is lacking. This study aimed to incorporate individualized and predictive measurements of the liver maximum capacity (LiMAx) test to objectively grade liver function during aNRP and prevent post-op complications.
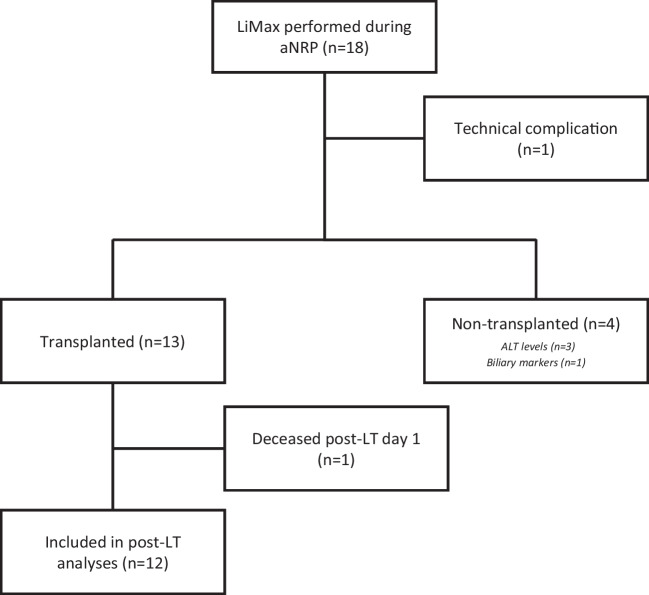
aNRP was performed to salvage 18 DCD liver grafts, otherwise discarded. Continuous variables were presented as the median with the interquartile range.
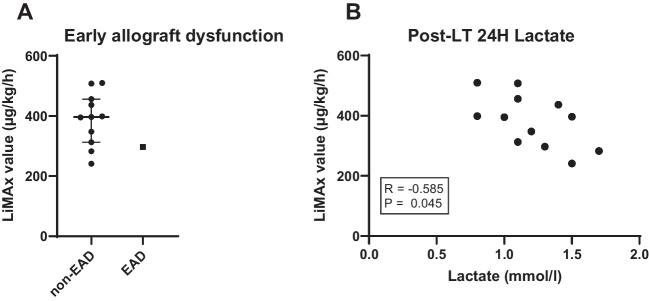
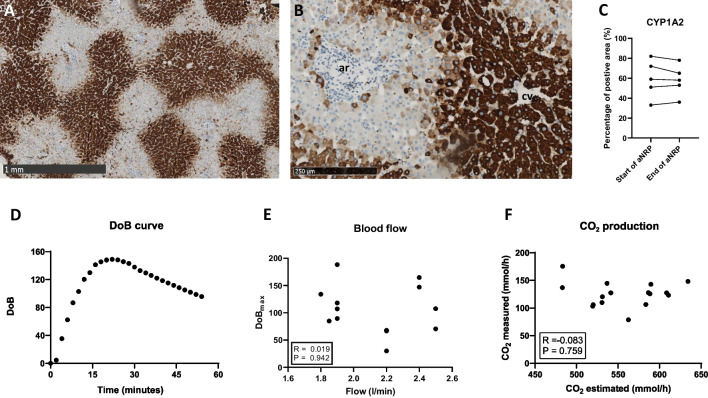
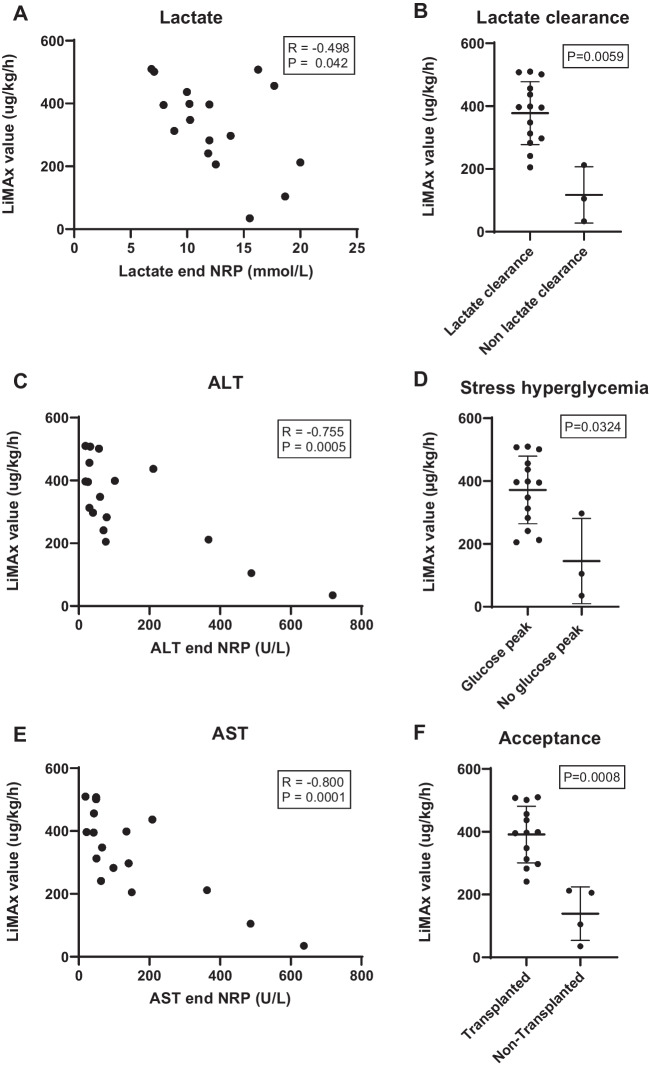
The liver function maximum capacity (LiMAx) test was successfully performed within the aNRP circuit in 17 aNRPs (94%). Donor livers with good lactate clearance during aNRP demonstrated significantly higher LiMAx scores (396 (301-451) µg/kg/h versus those who did not 105 (70-158) µg/kg/h; = 0.006). This was also true for manifesting stress hyperglycemia > 20 mmol/l ( = 0.032). LiMAx score correlated with alanine aminotransferase (ALT; = - 0.755) and aspartate transaminase (AST; = - 0.800) levels during perfusion and distinguished livers that were selected for transplantation (397 (346-453) µg/kg/h) from those who were discarded (155 (87-206) µg/kg/h; < 0.001). Twelve livers were accepted for transplantation, blinded for LiMAx results, and all had LiMAx scores of > 241 µg/kg/h. Postoperatively, LiMAx during aNRP displayed correlation with 24-h lactate levels.
This study shows for the first time the feasibility to assess liver function during aNRP in individual donor livers. LiMAx presents an objective tool to predict donor liver function and risk of complications in the recipient, thus enabling individualized matching of donor livers for an individual recipient. The LiMAx test may present a valuable test for the prediction of donor liver function, preventing post-transplant complication, and personalizing the selection of donor livers for individual recipients.
The online version contains supplementary material available at 10.1007/s13167-024-00371-7.
为降低等待名单上的死亡率,包括循环死亡后捐赠(DCD)器官在内的扩大标准供体器官的使用频率日益增加。这些供体术后并发症风险增加,目前平衡供体-受体风险是基于通用的列线图。腹部常温区域灌注(aNRP)能够对DCD器官进行个体评估,但缺乏确定移植适用性的金标准。本研究旨在纳入肝脏最大能力(LiMAx)测试的个体化和预测性测量,以在aNRP期间客观分级肝功能并预防术后并发症。
进行aNRP以挽救18个原本会被丢弃的DCD肝移植供体肝脏。连续变量以中位数和四分位间距表示。
在17次aNRP(94%)中,LiMAx测试在aNRP回路内成功进行。在aNRP期间乳酸清除良好的供体肝脏显示出显著更高的LiMAx评分(396(301 - 451)μg/kg/h,而未良好清除乳酸的为105(70 - 158)μg/kg/h;P = 0.006)。对于出现应激性高血糖>20 mmol/l的情况也是如此(P = 0.032)。LiMAx评分与灌注期间的丙氨酸氨基转移酶(ALT;P = -0.755)和天冬氨酸氨基转移酶(AST;P = -0.800)水平相关,并区分了被选用于移植的肝脏(397(346 - 453)μg/kg/h)和被丢弃的肝脏(155(87 - 206)μg/kg/h;P < 0.001)。12个肝脏被接受用于移植,对LiMAx结果不知情,且所有肝脏的LiMAx评分均>241 μg/kg/h。术后,aNRP期间的LiMAx与24小时乳酸水平相关。
本研究首次表明在个体供体肝脏的aNRP期间评估肝功能的可行性。LiMAx提供了一种客观工具,可预测供体肝功能和受体并发症风险,从而实现供体肝脏与个体受体的个体化匹配。LiMAx测试可能是预测供体肝功能、预防移植后并发症以及为个体受体个性化选择供体肝脏的有价值测试。
在线版本包含可在10.1007/s13167 - 024 - 00371 - 7获取的补充材料。