Department of Hematology, Qilu Hospital of Shandong University, 107 West Wenhua Road, Jinan, Shandong, 250012, China.
North China University of Science and Technology Affiliated Hospital, Tangshan, China.
Diagn Pathol. 2024 Sep 7;19(1):122. doi: 10.1186/s13000-024-01544-8.
Post-transplant lymphoproliferative disorders (PTLD) are rare but severe complications that occur after solid organ or allogeneic hematopoietic stem cell transplantations (allo-HSCT), with rapid progression and high mortality. Primary central nervous system (CNS)-PTLD are rarely recognized histo-pathologically. In addition, the diagnostic value of the Epstein-Barr virus (EBV) DNA copies in CNS-PTLD remains poorly understood.
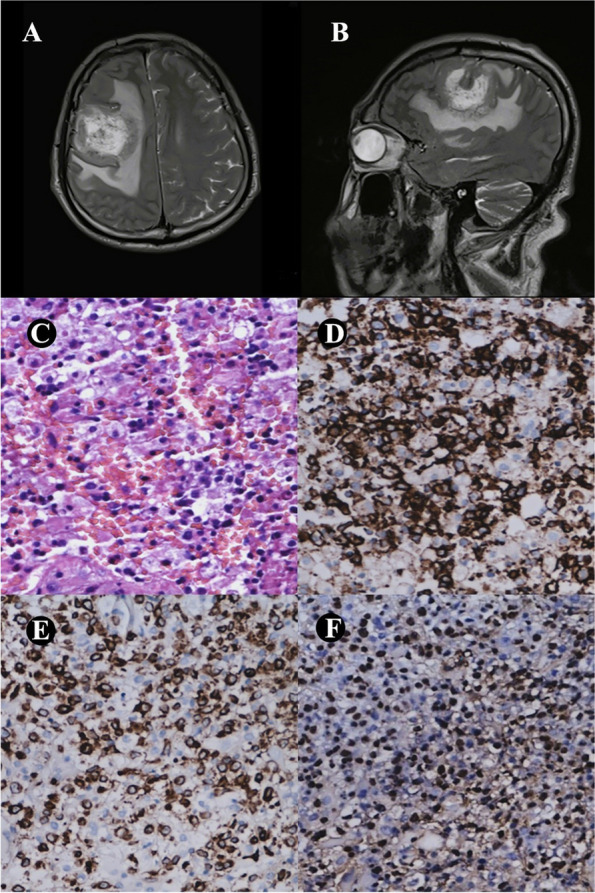
We herein report a case of monomorphic EBV-associated CNS-PTLD (diffuse large B-cell lymphoma, DLBCL) after allo-HSCT and perform a meta-analysis to assess the efficacy of PTLD treatment strategies in recent years.
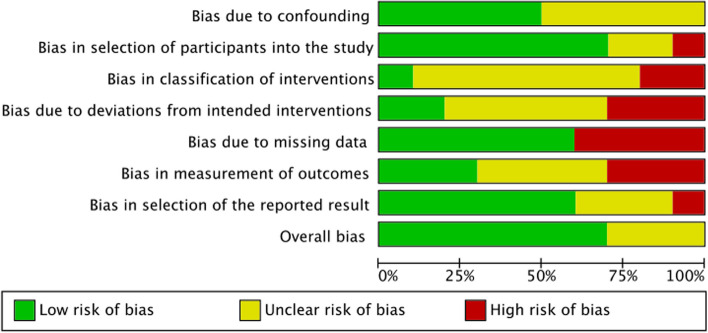
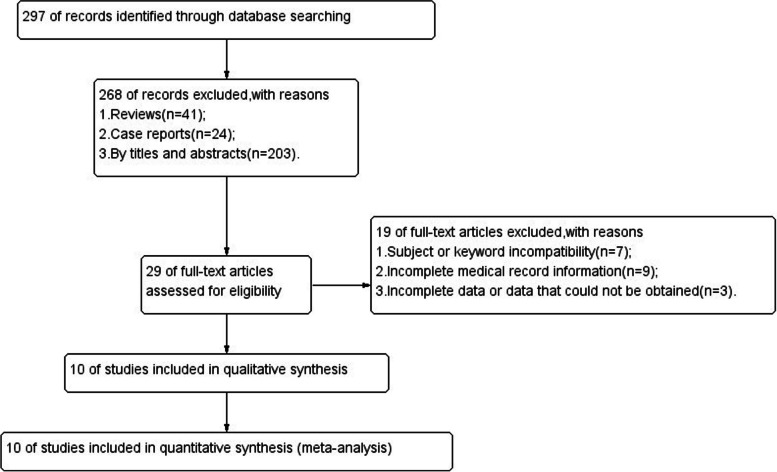
We present the case report covering clinical manifestations, diagnosis, treatment, and outcomes of a patient with primary CNS-PTLD. Additionally, we include a systematic review and meta-analysis of the clinical characteristics of 431 patients with PTLD after allo-HSCT. We evaluate the main treatment options and outcomes of PTLD management, including rituximab, chemotherapies, and autologous or human leukocyte antigen (HLA)-matched EBV-specific cytotoxic T lymphocyte infusion (EBV-CTLs)/donor lymphocyte infusion (DLI).
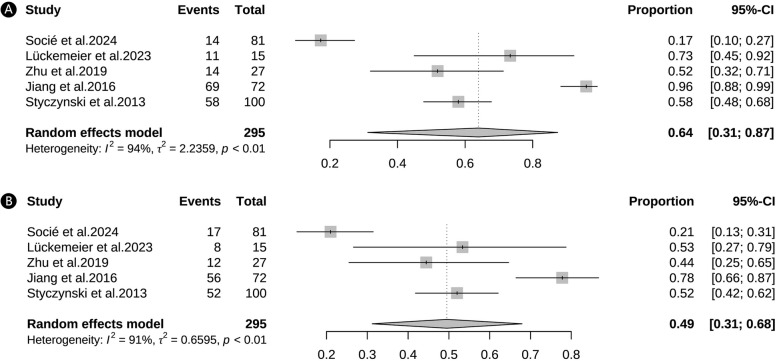
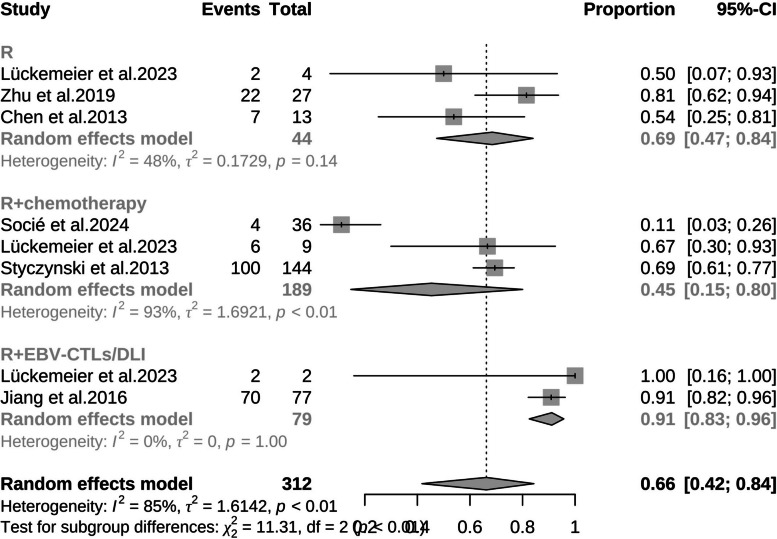
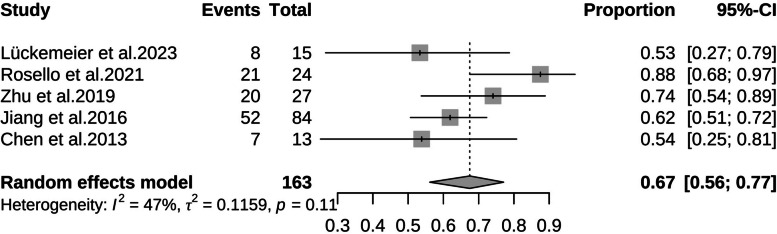
The meta-analysis revealed an overall response rate of 69.0% for rituximab alone (95% CI: 0.47-0.84), 45.0% for rituximab plus chemotherapies (95% CI: 0.15-0.80), and 91.0% for rituximab plus EBV-CTLs/DLI (95% CI: 0.83-0.96). The complete response (CR) rate after treatments for PTLD was 67.0% (95% CI: 0.56-0.77). Moreover, the 6-month and 1-year overall survival (OS) rate was 64.0% (95% CI: 0.31-0.87) and 49.0% (95% CI: 0.31-0.68), respectively.
This case highlighted the urgent need for effective, low-toxic treatment regimens for CNS-PTLD. Our meta-analysis suggested that rituximab combined with EBV-CTLs/DLI could be a favorable strategy for the management of PTLD after allo-HSCT.
移植后淋巴组织增生性疾病(PTLD)是实体器官或异基因造血干细胞移植(allo-HSCT)后罕见但严重的并发症,其进展迅速,死亡率高。原发性中枢神经系统(CNS)-PTLD 在组织病理学上很少被认识到。此外,CNS-PTLD 中 EBV 病毒(EBV)DNA 拷贝的诊断价值仍知之甚少。
我们在此报告一例 allo-HSCT 后发生的单形性 EBV 相关 CNS-PTLD(弥漫性大 B 细胞淋巴瘤,DLBCL),并进行荟萃分析评估近年来 PTLD 治疗策略的疗效。
我们提出了一例原发性 CNS-PTLD 患者的病例报告,涵盖了临床表现、诊断、治疗和结局。此外,我们还对 allo-HSCT 后 431 例 PTLD 患者的临床特征进行了系统评价和荟萃分析。我们评估了 PTLD 管理的主要治疗选择和结局,包括利妥昔单抗、化疗以及自体或人类白细胞抗原(HLA)匹配的 EBV 特异性细胞毒性 T 淋巴细胞输注(EBV-CTLs)/供体淋巴细胞输注(DLI)。
荟萃分析显示,利妥昔单抗单药治疗的总体缓解率为 69.0%(95%CI:0.47-0.84),利妥昔单抗联合化疗的缓解率为 45.0%(95%CI:0.15-0.80),利妥昔单抗联合 EBV-CTLs/DLI 的缓解率为 91.0%(95%CI:0.83-0.96)。PTLD 治疗后的完全缓解(CR)率为 67.0%(95%CI:0.56-0.77)。此外,6 个月和 1 年的总生存率(OS)分别为 64.0%(95%CI:0.31-0.87)和 49.0%(95%CI:0.31-0.68)。
本病例强调了需要为 CNS-PTLD 制定有效、低毒的治疗方案。我们的荟萃分析表明,利妥昔单抗联合 EBV-CTLs/DLI 可能是 allo-HSCT 后治疗 PTLD 的一种有利策略。