Department of Neurology, University Hospital, Ludwig-Maximilians-University, Munich, Germany.
German Center for Vertigo and Balance Disorders, University Hospital, Ludwig-Maximilians-University, Munich, Germany.
Brain Behav. 2024 Sep;14(9):e70000. doi: 10.1002/brb3.70000.
Uni- or bilateral peripheralvestibular impairment causes objective spatial orientation deficits, which can be measured using pen-and-paper-tests or sensorimotor tasks (navigation or pointing). For patients' subjective orientation abilities, questionnaires are commonly used (e.g., Santa Barbara sense of direction scale [SBSODS]). However, the relationship between subjective assessment of spatial skills and objective vestibular function has only been scarcely investigated.
A total of 177 patients (mean age 57.86 ± 17.53 years, 90 females) who presented in our tertiary Center for Vertigo and Balance Disorders underwent neuro-otological examinations, including bithermal water calorics, video head impulse test (vHIT), and testing of the subjective visual vertical (SVV), and filled out the SBSODS (German version). Correlation analyses and linear multiple regression model analyses were performed between vestibular test results and self-assessment scores. Additionally, groupwise vestibular function for patients with low, average, and high self-report scores was analyzed.
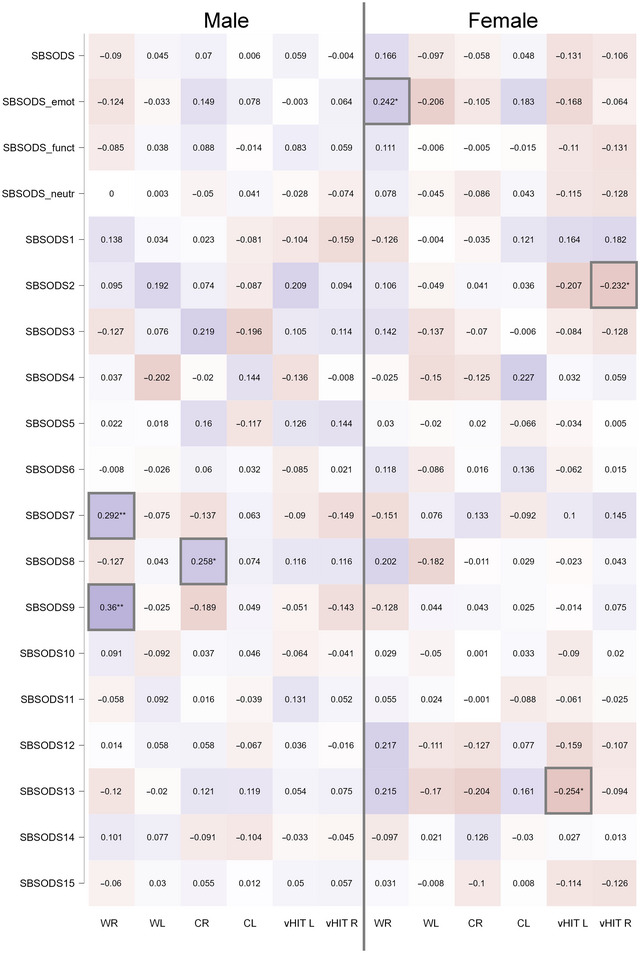
Forty-two patients fulfilled the diagnostic criteria for bilateral vestibulopathy, 93 for chronic unilateral vestibulopathy (68 unilateral caloric hypofunction and 25 isolated horizontal vestibulo-ocular reflex deficits), and 42 patients had normal vestibular test results. SBSODS scores showed clear sex differences with higher subjective skill levels in males (mean score males: 4.94 ± 0.99, females 4.40 ± 0.94; Student's t-test: t-3.78, p < .001***). No stable correlation between objective vestibular function and subjective sense of spatial orientation was found. A multiple linear regression model could not reliably explain the self-reported variance. The three patient groups with low, average, and high self-assessment-scores showed no significant differences of vestibular function.
Self-reported assessment of spatial orientation does not robustly correlate with objective peripheral vestibular function. Therefore, other methods of measuring spatial skills in real-world and virtual environments are required to disclose orientation deficits due to vestibular hypofunction.
单侧或双侧外周前庭功能障碍会导致客观的空间定向障碍,这些障碍可以通过纸笔测试或感觉运动任务(导航或指向)来测量。对于患者的主观定向能力,通常使用问卷进行评估(例如,圣巴巴拉方向感量表 [SBSODS])。然而,主观评估空间技能与客观前庭功能之间的关系仅得到了很少的研究。
共有 177 名患者(平均年龄 57.86 ± 17.53 岁,90 名女性)在我们的三级眩晕和平衡障碍中心接受了神经耳科检查,包括双侧冷热水测听、视频头脉冲试验(vHIT)和主观垂直视觉(SVV)测试,并填写了 SBSODS(德语版)。对前庭测试结果与自我评估评分之间进行了相关分析和线性多元回归模型分析。此外,还对自我报告评分低、中、高的患者进行了分组前庭功能分析。
42 名患者符合双侧前庭病变的诊断标准,93 名患者符合慢性单侧前庭病变(68 名单侧热刺激测听减退,25 名孤立性水平前庭眼反射减退),42 名患者的前庭测试结果正常。SBSODS 评分存在明显的性别差异,男性的主观技能水平较高(男性平均评分:4.94 ± 0.99,女性 4.40 ± 0.94;学生 t 检验:t=-3.78,p<.001***)。客观前庭功能与主观空间定向感之间没有稳定的相关性。多元线性回归模型不能可靠地解释自我报告的方差。自我评估得分低、中、高的三组患者的前庭功能无显著差异。
自我报告的空间定向评估与客观外周前庭功能没有很强的相关性。因此,需要在现实和虚拟环境中使用其他方法来测量空间技能,以揭示由于前庭功能减退导致的定向障碍。