Nelles Christian, Gräf Moritz, Bernard Pascale, Persigehl Thorsten, Große Hokamp Nils, Zopfs David, Maintz David, Kreuzberg Nicole, Wolf Jürgen, Bröckelmann Paul J, Lennartz Simon
Institute for Diagnostic and Interventional Radiology, Faculty of Medicine and University Hospital Cologne, University of Cologne, Cologne, Germany.
Department I of Internal Medicine, Center for Integrated Oncology Aachen Bonn Cologne Düsseldorf (CIO ABCD), Faculty of Medicine and University Hospital Cologne, University of Cologne, Cologne, Germany.
Eur Radiol. 2025 Apr;35(4):2084-2093. doi: 10.1007/s00330-024-11060-4. Epub 2024 Sep 18.
To compare immune response evaluation criteria in solid tumors (iRECIST) and response evaluation criteria in solid tumors (RECIST) 1.1 for response assessment of immune checkpoint inhibitor (ICI) therapy in a real-world setting in patients with melanoma and non-small cell lung cancer (NSCLC).
Two-hundred fifty-two patients with melanoma and NSCLC who received CTLA-4 inhibitor ipilimumab or PD-1 inhibitors nivolumab or pembrolizumab and who underwent staging CT of the chest and abdomen were retrospectively included. Treatment response evaluation according to the RECIST 1.1 and iRECIST guidelines was performed for all patients. Response patterns, as well as overall response rate (ORR), disease control rate (DCR), and time to progression (TTP), were compared between RECIST 1.1 and iRECIST.
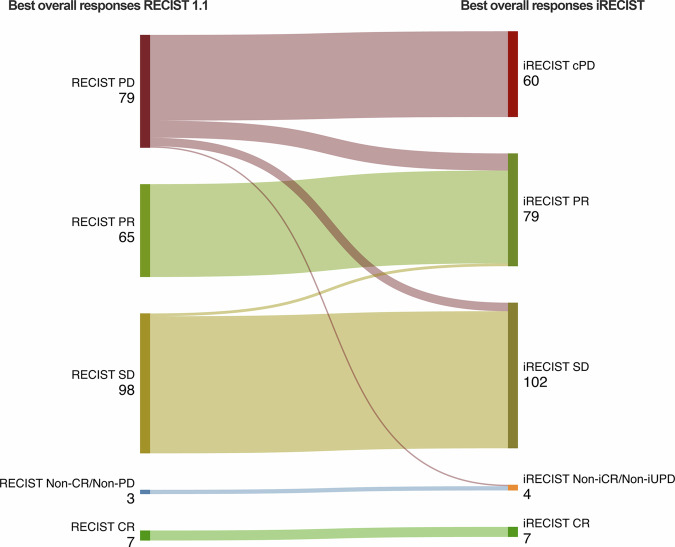
Out of 143 patients with progressive disease (PD) according to RECIST 1.1, 48 (33.6%) did not attain confirmation of progression (iCPD) as per iRECIST and six patients who were treated beyond RECIST 1.1 progression reached PD at a later point in time in iRECIST, resulting in a significant difference in TTP between iRECIST and RECIST 1.1 (618.3 ± 626.9 days vs. 538.1 ± 617.9 days, respectively (p < 0.05)). The number of non-responders as per RECIST 1.1 was 79, whereas it was 60 when using iRECIST. ORR was 28.5% for RECIST 1.1 and 34.1% for iRECIST, and corresponding DCR of 67.4% for RECIST 1.1 and 74.6% for iRECIST.
iRECIST was more suitable than RECIST 1.1 for capturing atypical response patterns to ICI therapy in patients with melanoma and NSCLC, resulting in differences in the assessment of treatment response.
Compared to RECIST 1.1, iRECIST may improve patient care and treatment decisions for patients with NSCLC or melanoma who are treated with immune checkpoint inhibitors in clinical routine.
RECIST 1.1 may incorrectly assess atypical treatment patterns to immune checkpoint inhibitors. iRECIST better captured atypical response patterns compared to RECIST 1.1. iRECIST was more suitable for assessing response to immune checkpoint inhibitors in non-small cell lung carcinoma and melanoma.
比较实体瘤免疫反应评估标准(iRECIST)与实体瘤疗效评价标准(RECIST)1.1,以评估免疫检查点抑制剂(ICI)疗法在黑色素瘤和非小细胞肺癌(NSCLC)患者真实临床环境中的疗效。
回顾性纳入252例接受细胞毒性T淋巴细胞相关抗原4(CTLA-4)抑制剂伊匹单抗或程序性死亡受体1(PD-1)抑制剂纳武单抗或派姆单抗治疗且接受胸部和腹部分期CT检查的黑色素瘤和NSCLC患者。根据RECIST 1.1和iRECIST指南对所有患者进行治疗反应评估。比较RECIST 1.1和iRECIST之间的反应模式、总缓解率(ORR)、疾病控制率(DCR)和疾病进展时间(TTP)。
根据RECIST 1.1,143例疾病进展(PD)患者中,48例(33.6%)未达到iRECIST定义的疾病进展确认(iCPD),6例在RECIST 1.1定义的疾病进展后继续接受治疗的患者在iRECIST中于稍后时间点达到PD,导致iRECIST和RECIST 1.1之间TTP存在显著差异(分别为618.3±626.9天和538.1±617.9天,p<0.05)。根据RECIST 1.1,无反应者数量为79例,而使用iRECIST时为60例。RECIST 1.1的ORR为28.5%,iRECIST为34.1%,相应的RECIST 1.1的DCR为67.4%,iRECIST为74.6%。
对于黑色素瘤和NSCLC患者ICI治疗的非典型反应模式,iRECIST比RECIST 1.1更适合捕捉,导致治疗反应评估存在差异。
与RECIST 1.1相比,iRECIST可能改善临床常规接受免疫检查点抑制剂治疗的NSCLC或黑色素瘤患者的医疗护理和治疗决策。
RECIST 1.1可能错误评估免疫检查点抑制剂的非典型治疗模式。与RECIST 1.1相比,iRECIST能更好地捕捉非典型反应模式。iRECIST更适合评估非小细胞肺癌和黑色素瘤对免疫检查点抑制剂的反应。