Coz Yataco Angel O, Soghier Israa, Hébert Paul C, Belley-Cote Emilie, Disselkamp Margaret, Flynn David, Halvorson Karin, Iaccarino Jonathan M, Lim Wendy, Lindenmeyer Christina C, Miller Peter J, O'Neil Kevin, Pendleton Kathryn M, Vande Vusse Lisa, Ouellette Daniel R
Critical Care Medicine Division and Pulmonary Medicine Division, Integrated Hospital-Care Institute, Cleveland, OH; Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH.
Division of Pulmonary and Critical Care Medicine, Department of Medicine, Salem Hospital/Massachusetts General Brigham, Salem, MA; American College of Chest Physicians, Glenview, IL.
Chest. 2025 Feb;167(2):477-489. doi: 10.1016/j.chest.2024.09.016. Epub 2024 Sep 26.
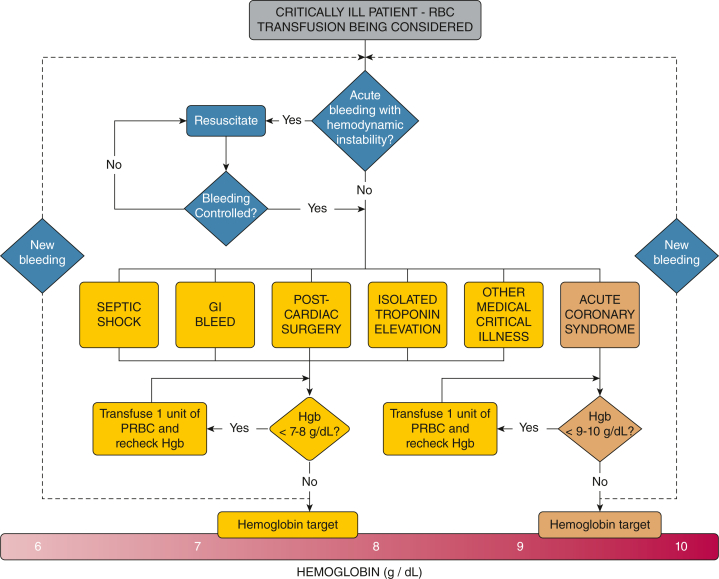
Blood products frequently are administered to critically ill patients. Considering recent trials and practice variability, a comprehensive review of current evidence was deemed essential to offer pertinent guidance to critical care practitioners. This American College of Chest Physicians (CHEST) guidelines panel examined the literature on RBC transfusions among critically ill patients overall and specific subgroups, including patients with gastrointestinal bleeding, acute coronary syndrome (ACS), cardiac surgery, isolated troponin elevation, and septic shock, to provide evidence-based recommendations.
A panel of experts developed six Population, Intervention, Comparator, and Outcome questions addressing RBC transfusions in critically ill patients and performed a comprehensive evidence review. The panel applied the Grading of Recommendations, Assessment, Development, and Evaluations approach to assess the certainty of evidence and to formulate and grade recommendations. A modified Delphi technique was used to reach consensus on the recommendations.
The initial search identified a total of 3,082 studies, and after the initial screening, 38 articles were reviewed. Among them, 23 studies met inclusion criteria, comprising 22 randomized controlled trials and one cohort study. Based on the analysis of these studies, the panel formulated two strong and four conditional recommendations. The overall quality of evidence for recommendations ranged from very low to moderate.
In most critically ill patients, a restrictive strategy was preferable to a permissive approach because it does not increase the risk of death or complications, but does decrease RBC use significantly. Data from critically ill subpopulations also supported a restrictive approach, except in patients with ACS, for whom favoring a restrictive approach could increase adverse outcomes.
血液制品经常被用于重症患者。鉴于近期的试验和实践差异,对当前证据进行全面回顾被认为对于为重症监护从业者提供相关指导至关重要。美国胸科医师学会(CHEST)的这个指南小组审查了关于重症患者总体以及特定亚组(包括胃肠道出血患者、急性冠脉综合征(ACS)患者、心脏手术患者、单纯肌钙蛋白升高患者和感染性休克患者)红细胞输血的文献,以提供基于证据的建议。
一个专家小组针对重症患者红细胞输血提出了六个“人群、干预措施、对照和结局”问题,并进行了全面的证据回顾。该小组采用推荐分级、评估、制定和评价方法来评估证据的确定性,并制定和分级建议。采用改良的德尔菲技术就这些建议达成共识。
初步检索共识别出3082项研究,经过初步筛选,对38篇文章进行了审查。其中,23项研究符合纳入标准,包括22项随机对照试验和1项队列研究。基于对这些研究的分析,该小组制定了两项强烈推荐和四项有条件推荐。推荐建议的证据总体质量从极低到中等不等。
在大多数重症患者中,限制性策略优于宽松策略,因为它不会增加死亡或并发症风险,但会显著减少红细胞的使用。重症亚组人群的数据也支持采用限制性方法,但ACS患者除外,对ACS患者采用限制性方法可能会增加不良结局。