Sim Marcus, Sharma Vibha, Li Karen, Gowland Mary Hazel, Garcez Tomaz, Shilladay Cassandra, Pumphrey Richard, Patel Nandinee, Turner Paul J, Boyle Robert J
National Heart and Lung Institute, Imperial College London, London, UK.
Royal Manchester Children's Hospital, Manchester, UK.
Clin Exp Allergy. 2025 Jan;55(1):19-35. doi: 10.1111/cea.14565. Epub 2024 Oct 9.
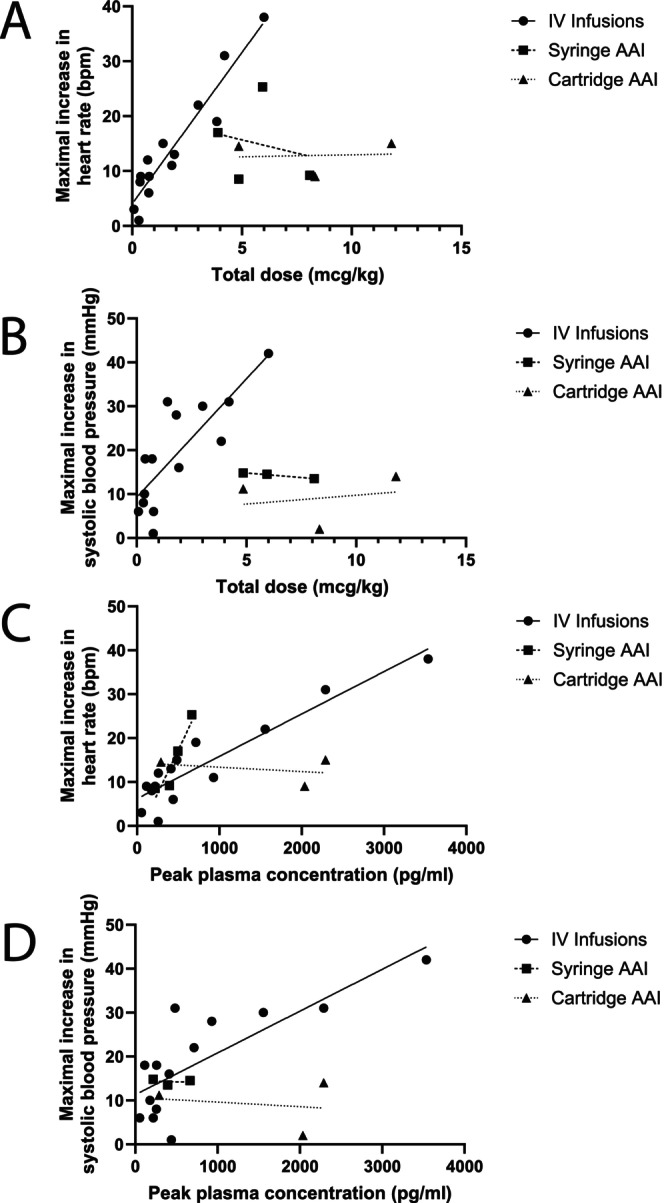
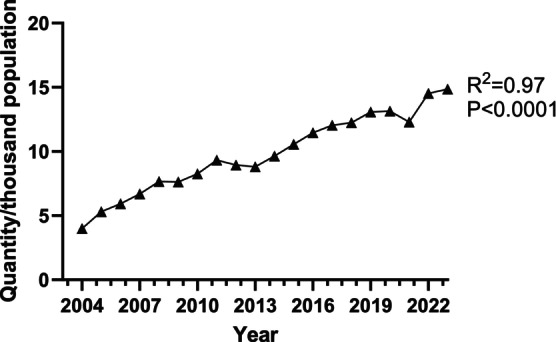
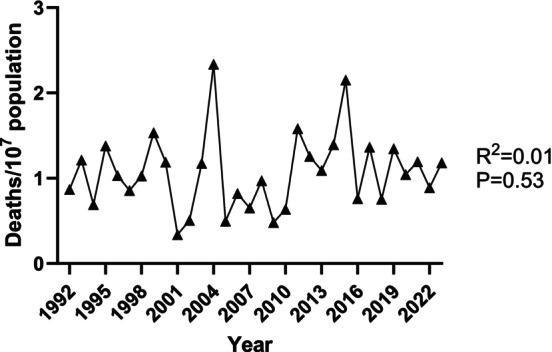
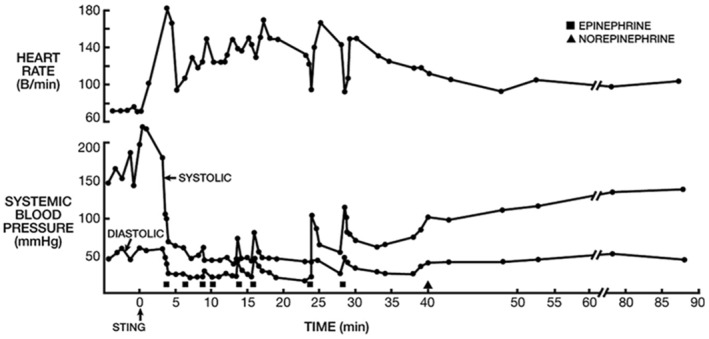
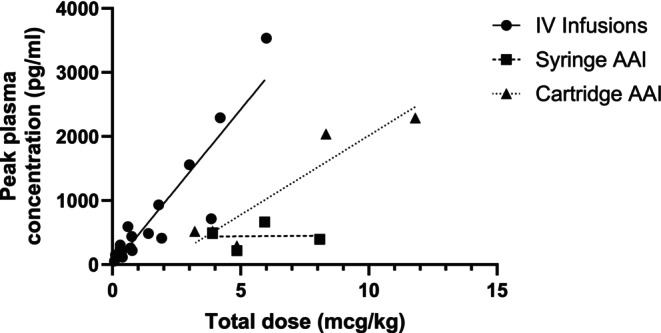
Anaphylaxis affects up to 5% of people during their lifetime. Although anaphylaxis usually resolves without long-term physical consequences, it can result in anxiety and quality of life impairment. Rarely and unpredictably, community anaphylaxis can cause rapid physiological decompensation and death. Adrenaline (epinephrine) is the cornerstone of anaphylaxis treatment, and provision of adrenaline autoinjectors (AAI) has become a standard of care for people at risk of anaphylaxis in the community. In this article, we explore the effectiveness of AAIs for preventing fatal outcomes in anaphylaxis, using information drawn from animal and human in vivo studies and epidemiology. We find that data support the effectiveness of intravenous adrenaline infusions for reversing physiological features of anaphylaxis, typically at doses from 0.05 to 0.5 μg/kg/min for 1-2 h, or ~ 10 μg/kg total dose. Intramuscular injection of doses approximating 10 μg/kg in humans can result in similar peak plasma adrenaline levels to intravenous infusions, at 100-500 pg/mL. However, these levels are typically short-lived following intramuscular adrenaline, and pharmacokinetic and pharmacodynamic outcomes can be unpredictable. Epidemiological data do not support an association between increasing AAI prescriptions and reduced fatal anaphylaxis, although carriage and activation rates remain low. Taken together, these data suggest that current AAIs have little impact on rates of fatal anaphylaxis, perhaps due to a lack of sustained and sufficient plasma adrenaline concentration. Effects of AAI prescription on quality of life may be variable. There is a need to consider alternatives, which can safely deliver a sustained adrenaline infusion via an appropriate route.
一生中,多达5%的人会发生过敏反应。虽然过敏反应通常可自行缓解,不会产生长期身体后果,但可能导致焦虑和生活质量受损。在社区中,过敏反应极少且不可预测地会导致快速的生理代偿失调和死亡。肾上腺素是过敏反应治疗的基石,为有社区过敏反应风险的人提供肾上腺素自动注射器已成为一种护理标准。在本文中,我们利用从动物和人体体内研究及流行病学中获取的信息,探讨肾上腺素自动注射器预防过敏反应致命后果的有效性。我们发现,数据支持静脉注射肾上腺素输注逆转过敏反应生理特征的有效性,通常剂量为0.05至0.5μg/kg/分钟,持续1 - 2小时,或总剂量约为10μg/kg。在人类中,肌肉注射近似10μg/kg的剂量可使血浆肾上腺素峰值水平与静脉输注相似,达到100 - 500pg/mL。然而,肌肉注射肾上腺素后,这些水平通常持续时间较短,药代动力学和药效学结果可能不可预测。流行病学数据不支持增加肾上腺素自动注射器处方与降低致命性过敏反应之间存在关联,尽管携带率和激活率仍然较低。综合来看,这些数据表明,目前的肾上腺素自动注射器对致命性过敏反应发生率影响不大,可能是由于缺乏持续且足够高的血浆肾上腺素浓度。肾上腺素自动注射器处方对生活质量的影响可能因人而异。有必要考虑替代方案,这些方案可以通过适当途径安全地提供持续的肾上腺素输注。