Tejedor Ana, Bijelic Lana, García Marta
Department of Anesthesiology, Hospital Sant Joan Despí Moisès Broggi, Barcelona, Spain.
Department of Surgery, Hospital Sant Joan Despí Moisès Broggi, Barcelona, Spain.
J Anaesthesiol Clin Pharmacol. 2024 Jul-Sep;40(3):523-529. doi: 10.4103/joacp.joacp_375_23. Epub 2024 Apr 8.
Opioid-free anesthesia (OFA) provides adequate analgesia minimizing opioids. OFA has not been evaluated in laparoscopic radical prostatectomy (LRP). Our aim was to evaluate OFA feasibility and its effectiveness in LRP.
A quasi-experimental retrospective study of 55 adult patients undergoing LRP was performed from September 2020 until December 20223. Predefined protocols for either opioid-based anesthesia (OBA; with continuous remifentanil infusion) or OFA (continuous lidocaine, dexmedetomidine, and ketamine infusion) were followed. In both groups, wound infiltration was performed before skin incision. Primary outcome was postoperative pain management (numerical rating scale [NRS]) in the first 24 postoperative hours. Secondary outcomes were opioid consumption, start to sitting and ambulation, postoperative complications, and length of hospital stay.
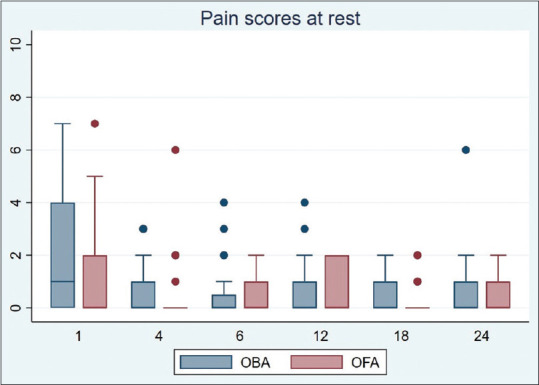
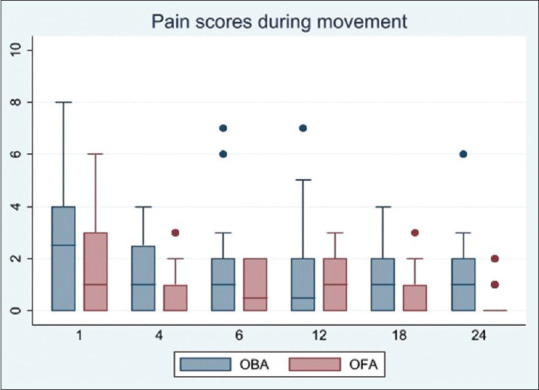
OFA protocol patients had better median pain scores during movement at 1, 18 and 24 h, that is, 1 (interquartile range [IQR] 0-3) versus 2.5 (IQR 0-4), = 0.047; 0 (IQR 0-1) versus 1 (IQR 0-2), = 0.017; and 0 (IQR 0-0.25) versus 1 (IQR 0-2), = 0.013, respectively. At 6 and 12 h, there were no statistically significant differences, that is, 0.5 (IQR 0-2) versus 1 (IQR 0-2), = 0.908 and 1 (IQR 0-2) versus 0.5 (IQR 0-2), = 0.929, respectively. Lower morphine requirements were recorded in the first 18 and 24 postoperative hours, that is, 0 (IQR 0-0) versus 1 (IQR 0-2.75) mg, = 0.028 and 0 (IQR 0-2) versus 1.5 (IQR 0-3) mg, = 0.012, respectively. Start to sitting and ambulation occurred earlier in the OFA group ( = 0.030 and = 0.002, respectively). Linear regression showed that ambulation was independently associated with the analgesic technique ( = 0.034). Only one patient had postoperative nausea and vomiting (PONV) and belonged to the OBA group. There was no difference in total complications or the length of stay.
In this study, OFA strategy was found to be safe, feasible, and provided adequate analgesia, minimizing the use of postoperative opioids, and was independently associated with earlier ambulation.
无阿片类麻醉(OFA)可提供充分镇痛并尽量减少阿片类药物的使用。尚未在腹腔镜前列腺癌根治术(LRP)中对OFA进行评估。我们的目的是评估OFA在LRP中的可行性及其有效性。
对2020年9月至2022年12月期间接受LRP的55例成年患者进行了一项准实验性回顾性研究。遵循基于阿片类药物的麻醉(OBA;持续输注瑞芬太尼)或OFA(持续输注利多卡因、右美托咪定和氯胺酮)的预定义方案。两组均在皮肤切口前进行伤口浸润。主要结局是术后24小时内的术后疼痛管理(数字评分量表[NRS])。次要结局包括阿片类药物消耗量、开始坐立和行走的时间、术后并发症及住院时间。
OFA方案组患者在术后1小时、18小时和24小时活动期间的中位疼痛评分更好,即分别为1(四分位间距[IQR]0 - 3)对2.5(IQR 0 - 4),P = 0.047;0(IQR 0 - 1)对1(IQR 0 - 2),P = 0.017;以及0(IQR 0 - 0.25)对1(IQR 0 - 2),P = 0.013。在术后6小时和12小时,无统计学显著差异,即分别为0.5(IQR 0 - 2)对1(IQR 0 - 2),P = 0.908和1(IQR 0 - 2)对0.5(IQR 0 - 2),P = 0.929。术后18小时和24小时记录到较低的吗啡需求量,即分别为0(IQR 0 - 0)对1(IQR 0 - 2.75)mg,P = 0.028和0(IQR 0 - 2)对1.5(IQR 0 - 3)mg,P = 0.012。OFA组开始坐立和行走的时间更早(分别为P = 0.030和P = 0.002)。线性回归显示行走与镇痛技术独立相关(P = 0.034)。仅1例患者发生术后恶心呕吐(PONV),且属于OBA组。总并发症或住院时间无差异。
在本研究中,发现OFA策略安全、可行,可提供充分镇痛,尽量减少术后阿片类药物的使用,且与更早行走独立相关。