National Institute for Health and Medical Research, (INSERM), UMR 1219, Research Institute for Sustainable Development (IRD), University of Bordeaux, Bordeaux Population Health Centre, EMR 271, Bordeaux, France.
Centre Hospitalier Universitaire de Bordeaux, Service de Médecine Interne et Maladies Infectieuses, Hôpital Saint-André, 1 rue Jean Burguet, 33075, Bordeaux, France.
Sci Rep. 2024 Oct 23;14(1):25028. doi: 10.1038/s41598-024-72449-1.
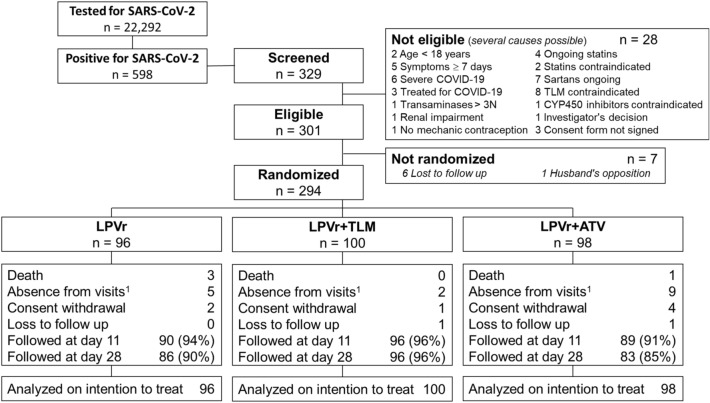
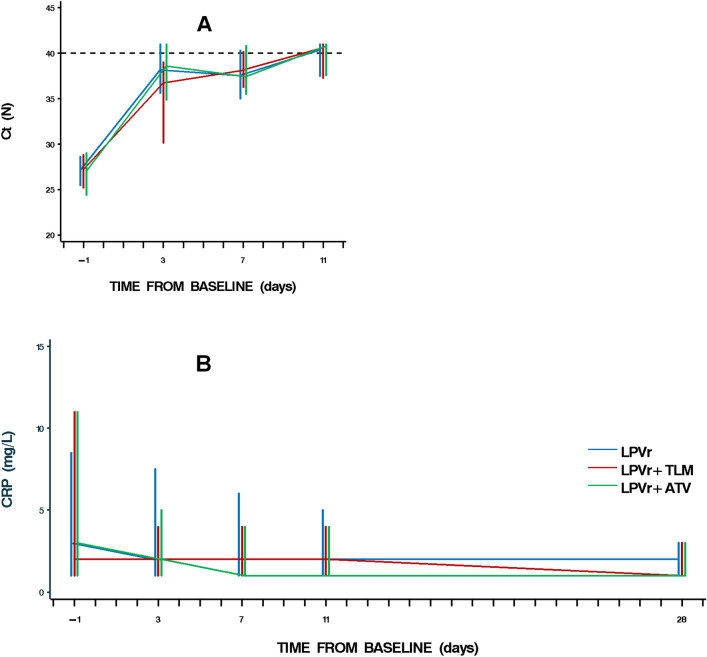
Observational studies suggest a reduction in fatal or severe COVID-19 disease with the use of ACE2 inhibitors and statins. We implemented a randomized controlled tree-arm open label trial evaluating the benefits of adding telmisartan (TLM) or atorvastatin (ATV) to lopinavir boosted ritonavir (LPVr) on the SARS-CoV-2 nasopharyngeal viral load in patients with mild / moderate COVID-19 infection in Côte d'Ivoire. RT-PCR positive COVID-19 patients ≥ 18 years, with general or respiratory symptoms for less than 7 days were randomized (1:1:1) to receive LPVr (400 mg/100 mg twice daily), LPVr + TLM (10 mg once daily) or LPVr + ATV (20 mg once daily) for 10 days. The primary endpoint was viro-inflammatory success defined as a composite variable at day 11: Ct ≥ 40 and C-reactive protein < 27 mg/L. We randomized 294 patients: 96 to LPVr, 100 to LPVr + TLM, 98 to LPVr + ATV arms. Baseline characteristics were well balanced between arms. In the primary analysis (missing = failure), 46% patients in the LPVr arm reached viro-inflammatory success at day 11 vs 43% in the LPVr + TLM arm (p = 0.69) and 43% in the LPVr + ATV arm (p = 0.68). The median time from baseline to resolution of COVID-19 related symptoms was not different between arms. Nine patients were hospitalized: 2 in the LPVr arm, 5 in the LPVr + TLM arm and 2 in the LPVr + ATV arm and 4 patients died. Among adults with mild to moderate COVID-19 infection, the addition of telmisartan or atorvastatin, to the standard LPVr treatment is not associated with a better virological or clinical outcome.Trial registration: NCT04466241, registered on 10/07/2020.
观察性研究表明,使用 ACE2 抑制剂和他汀类药物可以降低 COVID-19 重症或致死率。我们实施了一项随机对照三臂开放标签试验,评估在科特迪瓦轻度/中度 COVID-19 感染患者中,洛匹那韦利托那韦(LPVr)基础上加用替米沙坦(TLM)或阿托伐他汀(ATV)对 SARS-CoV-2 鼻咽部病毒载量的影响。纳入的患者均为 RT-PCR 阳性 COVID-19 患者,年龄≥18 岁,一般或呼吸道症状持续时间<7 天,按 1:1:1 随机分至 LPVr(400mg/100mg,每日 2 次)、LPVr+TLM(10mg,每日 1 次)或 LPVr+ATV(20mg,每日 1 次)治疗组,疗程 10 天。主要终点为第 11 天的病毒学和炎症反应成功,定义为复合变量:Ct≥40 和 C 反应蛋白(CRP)<27mg/L。共纳入 294 例患者,96 例进入 LPVr 组,100 例进入 LPVr+TLM 组,98 例进入 LPVr+ATV 组。各组间基线特征均衡。主要分析(缺失=失败)中,LPVr 组第 11 天病毒学和炎症反应成功的患者占 46%,LPVr+TLM 组为 43%(p=0.69),LPVr+ATV 组为 43%(p=0.68)。从基线到 COVID-19 相关症状缓解的中位时间在各组间无差异。9 例患者住院:LPVr 组 2 例,LPVr+TLM 组 5 例,LPVr+ATV 组 2 例,4 例患者死亡。在轻度至中度 COVID-19 感染的成年患者中,标准 LPVr 治疗基础上加用替米沙坦或阿托伐他汀,与病毒学或临床结局的改善无关。
NCT04466241,于 2020 年 7 月 10 日注册。