Richards Jarod A, Woodard David R, Kim H Mike
Department of Orthopaedic Surgery, Missouri Orthopaedic Institute, University of Missouri, Columbia, Missouri, U.S.A.
Arthrosc Tech. 2024 Jun 17;13(10):103073. doi: 10.1016/j.eats.2024.103073. eCollection 2024 Oct.
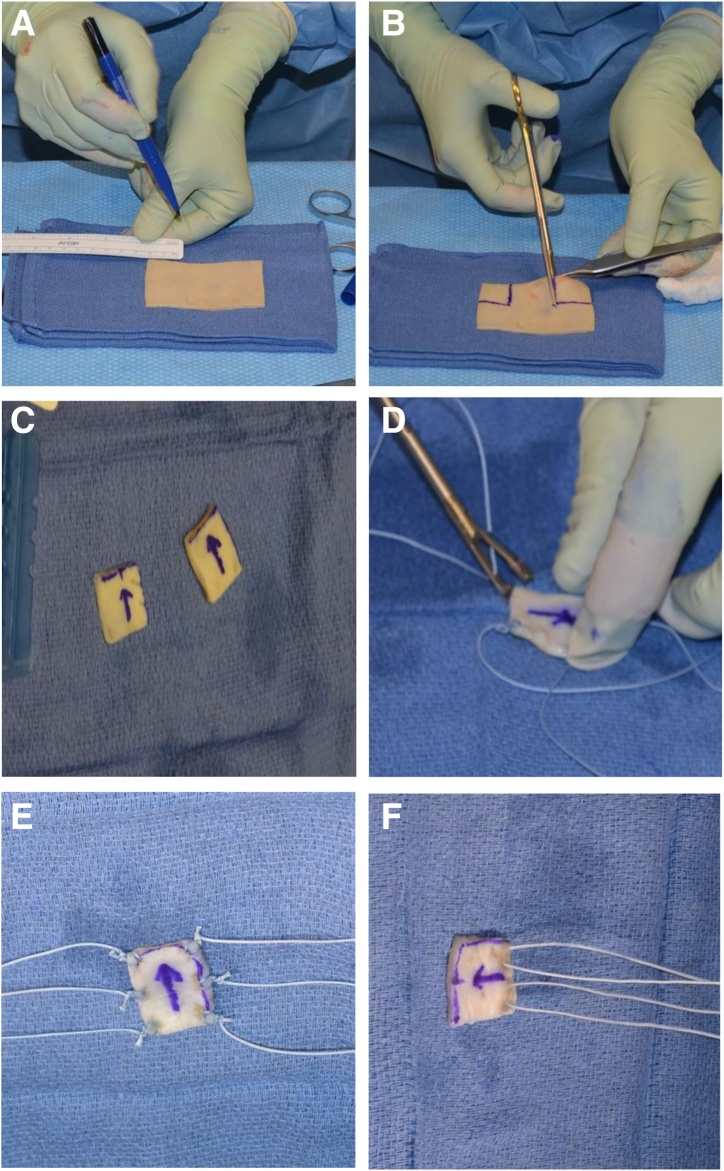
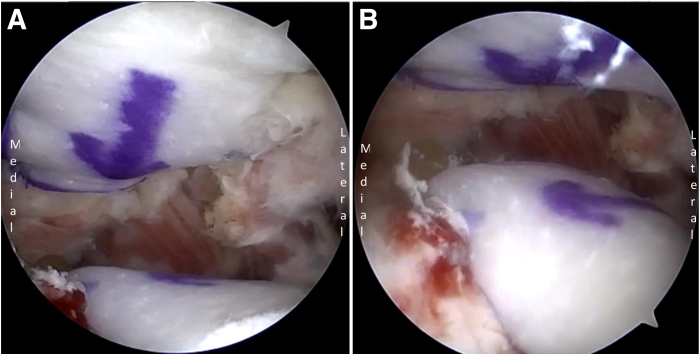
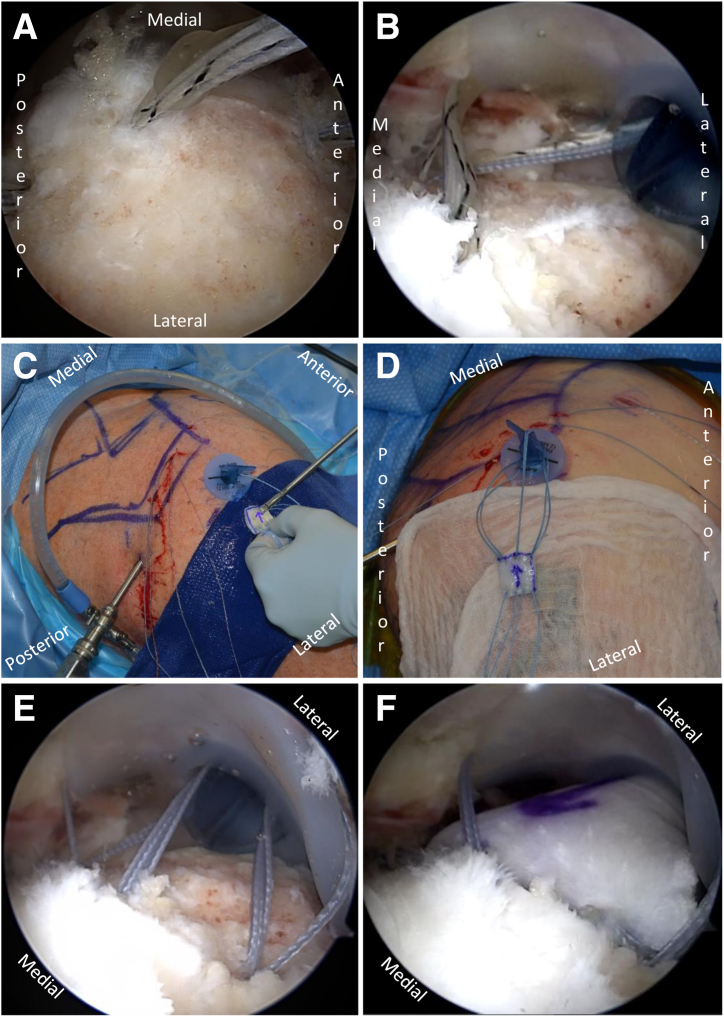
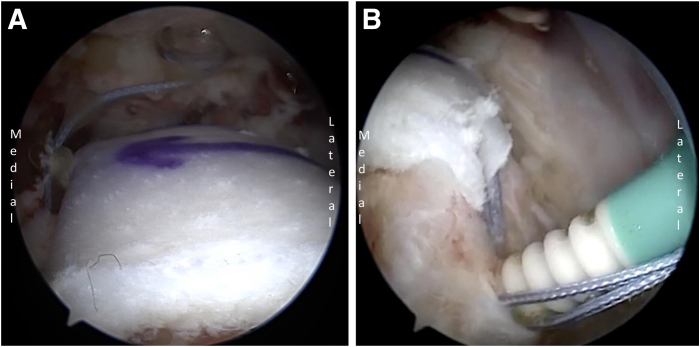
Recent attention has turned toward the prevention of acromiohumeral abutment in the treatment of irreparable rotator cuff tears (IRCTs). This can be achieved through tendon transfer with a bridging allograft, superior capsular reconstruction, dermal allograft application to the greater tuberosity (biologic tuberoplasty), bursal acromial reconstruction, or subacromial balloon spacer placement. Recent literature has demonstrated increased graft thickness is associated with improved clinical outcomes after superior capsular reconstruction, suggesting a potential role of a direct bone-to-bone contact between the greater tuberosity and acromion in symptom generation in patients with IRCTs. In keeping with this ethos and building on the principle of both biologic tuberoplasty and bursal acromial reconstruction, the authors propose biologic acromiotuberoplasty as a treatment for IRCTs wherein a 3-mm dermal allograft is fixated to both the greater tuberosity of the humerus and the undersurface of the acromion for a total of 6 mm of allograft interposition.
最近,在治疗不可修复的肩袖撕裂(IRCT)时,注意力已转向预防肩峰肱骨头撞击。这可以通过使用桥接同种异体移植物进行肌腱转移、上盂唇重建、将真皮同种异体移植物应用于大结节(生物结节成形术)、肩峰滑囊重建或肩峰下球囊间隔置入来实现。最近的文献表明,上盂唇重建后移植物厚度增加与临床结果改善相关,这表明在IRCT患者的症状产生中,大结节与肩峰之间的直接骨对骨接触可能起作用。本着这种精神,并基于生物结节成形术和肩峰滑囊重建的原则,作者提出生物肩峰结节成形术作为IRCT的一种治疗方法,即将一块3毫米的真皮同种异体移植物固定在肱骨大结节和肩峰下表面,总共置入6毫米的同种异体移植物。