Edinburgh Lung Fibrosis Clinic, Royal Infirmary of Edinburgh, Edinburgh, UK.
Department of Medicine, National Jewish Health, Denver, CO, USA.
BMC Pulm Med. 2024 Oct 31;24(1):547. doi: 10.1186/s12890-024-03287-0.
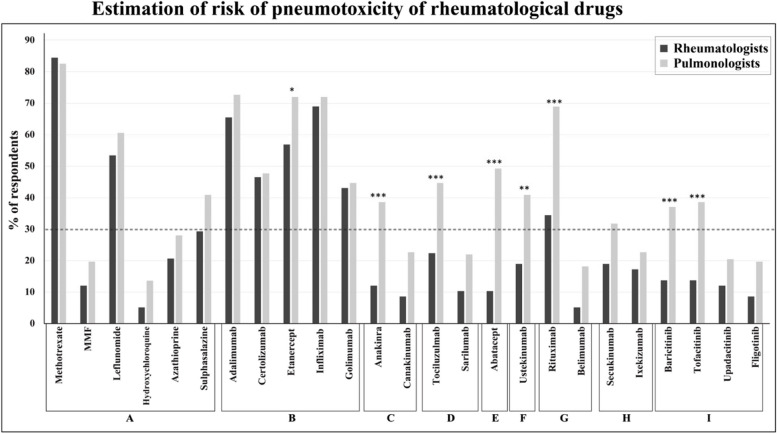
Drugs used to treat rheumatic disease are associated with pneumotoxicity (drug-induced lung disease), but little is known about associated risk factors.
To determine expert physician-perceived risk factors for developing pneumotoxicity in patients with rheumatologic conditions.
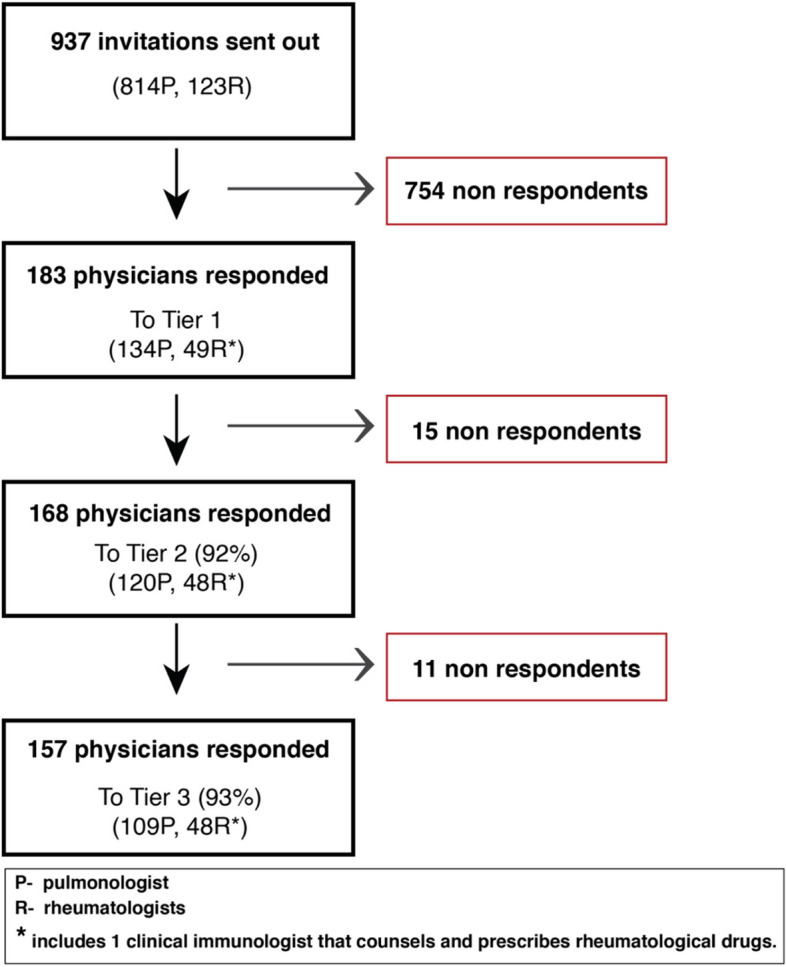
A modified international 3-tier Delphi exercise was performed. Tier 1 determined patient and drug variables that physicians perceive to be risk factors. Tier 2 determined degree of risk associated with the Tier-1 derived variables. Tier 3 aimed to internally validate and stratify exemplar cases into risk categories.
134 pulmonologists and 49 rheumatologists responded to Tier 1;157 physicians completed all tiers. Perceived risk factors included: drug type; history of previous pneumotoxicity; age; smoking; underlying rheumatic disease type and activity; renal function; pulmonary hypertension; left ventricular failure;presence, nature, severity and progression of pre-existing interstitial lung disease. Tier 2 data stratified these variables into risk profiles e.g. never versus current smoking was perceived as low and high risk respectively. An example of perceived high risk resulting from Tier 3 is a 75-year-old current smoker with high-activity rheumatoid arthritis (RA) with severe, progressive ILD being started on methotrexate. A perceived low risk is a 75-year-old currentsmoker with moderate-activity RA and emphysema with no cardiac or renal disease and no pre-existing ILD being started on rituximab. A risk prediction scoring tool is being developed to be used in validation studies.
This modified Delphi exercise defined and stratified the perceived risk factors for developing pneumotoxicity. Age, current smoking, high underlying rheumatological disease activity, HRCT definite UIP and honeycombing, severity and progression of pre-existing ILD were perceived to be the highest risk-factors.
治疗风湿性疾病的药物与肺毒性(药物引起的肺部疾病)有关,但对相关危险因素知之甚少。
确定风湿性疾病患者发生肺毒性的医师认为的危险因素。
采用改良的国际三级德尔菲法进行研究。第 1 层确定了医生认为是危险因素的患者和药物变量。第 2 层确定了与第 1 层得出的变量相关的风险程度。第 3 层旨在对内进行验证并将示例病例分层到风险类别中。
134 名肺病专家和 49 名风湿病专家对第 1 层做出了回应;157 名医生完成了所有 3 层的研究。感知到的危险因素包括:药物类型;既往肺毒性史;年龄;吸烟;潜在风湿性疾病类型和活动度;肾功能;肺动脉高压;左心衰竭;存在、性质、严重程度和进展性的预先存在的间质性肺病。第 2 层的数据将这些变量分层为风险概况,例如,当前吸烟与从不吸烟被认为是低风险和高风险。第 3 层感知到的高风险的一个例子是一位 75 岁的当前吸烟者,患有高活动度类风湿关节炎(RA),ILD 严重且进行性加重,开始接受甲氨蝶呤治疗。低风险的例子是一位 75 岁的当前吸烟者,患有中度活动度 RA 和肺气肿,没有心脏或肾脏疾病,没有预先存在的 ILD,开始接受利妥昔单抗治疗。正在开发风险预测评分工具,用于验证研究。
本改良德尔菲研究定义并分层了发生肺毒性的感知危险因素。年龄、当前吸烟、高基础风湿性疾病活动度、HRCT 明确的 UIP 和蜂窝肺、预先存在的 ILD 的严重程度和进展被认为是最高风险因素。