Khan Ayesha, Menon Raakhi, Corning Brooke, Cohn Steven, Kumfa Cecil, Raji Mukaila
Department of Internal Medicine, University of Texas at Medical Branch, 301 University Blvd, 5.138 RS, Galveston, TX 77555-5302, USA.
Department of Internal Medicine, University of Texas at Medical Branch, Galveston, TX, USA.
Therap Adv Gastroenterol. 2024 Oct 24;18:17562848241278125. doi: 10.1177/17562848241278125. eCollection 2024.
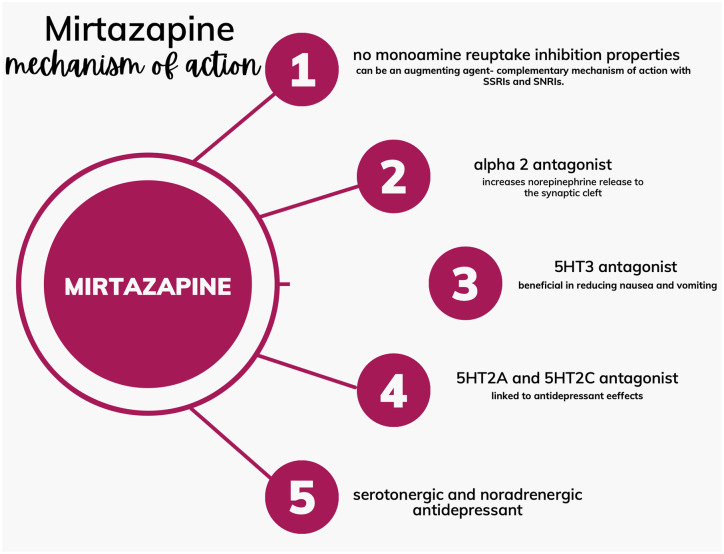
Irritable bowel syndrome (IBS) is a common and potentially modifiable contributor to excess disability, morbidity, and poor quality of life. Clinical trials of medications for IBS have largely been in younger adults. Yet, a growing number of adults aged 65 and older are living with IBS. No data exist to guide clinicians in the safe and effective use of medications (e.g., anticholinergics, anti-spasmodics, and tricyclic antidepressants (TCA)) for IBS in the geriatric population. These medications-especially anticholinergics and TCAs-carry a high risk of adverse effects (ADE) in older adults because of age-associated decline in drug metabolism and the high prevalence of multiple chronic conditions. Five or more medications (polypharmacy) are frequently used to treat common psychiatric and medical comorbidities of IBS: anxiety, depression, insomnia, migraine headache, diarrhea, nausea, poor appetite, pruritus/skin atopy, and fibromyalgia. These neurological and psychiatric comorbidities reflect shared pathogenic mechanisms and bidirectional crosstalk of high inflammation, alteration of gut microbiota, and dysregulation of multiple gastrointestinal and central nervous system-active neurotransmitters (e.g., serotonin, neuropeptides). Currently, these IBS-associated conditions are treated with multiple medications-which increase the risk of adverse drug-drug interactions. One way to reduce the number of medications used for IBS-associated conditions is the use of one medication that treats many or all of these conditions-Mirtazapine. In this perspective article, we present evidence from basic science, case series, observational and epidemiological studies, clinical studies, and clinical trials supporting mirtazapine, a noradrenergic and specific serotonergic receptor antagonist-with 5-hydroxytryptamine-2 and 3 antagonism, as a potential pharmacotherapeutic intervention for the myriad symptoms and conditions associated with IBS. Specifically, we found evidence of mirtazapine's role in treating diarrhea, insomnia, migraine headache, nausea, and poor appetite. We propose a large randomized controlled trial to study mirtazapine as a potential one-stop treatment for multiple IBS symptoms, with the potential to reduce polypharmacy and ADEs, especially in the geriatric population.
肠易激综合征(IBS)是导致残疾、发病和生活质量下降的常见且可能可改善的因素。IBS药物的临床试验主要针对年轻人。然而,越来越多65岁及以上的成年人患有IBS。目前尚无数据指导临床医生在老年人群中安全有效地使用治疗IBS的药物(如抗胆碱能药、抗痉挛药和三环类抗抑郁药(TCA))。由于药物代谢随年龄增长而下降以及多种慢性病的高患病率,这些药物,尤其是抗胆碱能药和三环类抗抑郁药,在老年人中具有较高的不良反应(ADE)风险。经常使用五种或更多药物(多重用药)来治疗IBS常见的精神和医学合并症:焦虑、抑郁、失眠、偏头痛、腹泻、恶心、食欲不振、瘙痒/皮肤过敏和纤维肌痛。这些神经和精神合并症反映了共同的致病机制以及高炎症、肠道微生物群改变和多种胃肠及中枢神经系统活性神经递质(如血清素、神经肽)失调之间的双向相互作用。目前,这些与IBS相关的病症采用多种药物治疗,这增加了药物间不良相互作用的风险。减少用于治疗与IBS相关病症的药物数量的一种方法是使用一种能治疗许多或所有这些病症的药物——米氮平。在这篇观点文章中,我们展示了来自基础科学、病例系列、观察性和流行病学研究、临床研究以及临床试验的证据,支持米氮平作为一种潜在的药物治疗干预手段,用于治疗与IBS相关的众多症状和病症。米氮平是一种去甲肾上腺素能和特异性5-羟色胺能受体拮抗剂,具有5-羟色胺-2和3拮抗作用。具体而言,我们发现了米氮平在治疗腹泻、失眠、偏头痛、恶心和食欲不振方面作用的证据。我们提议开展一项大型随机对照试验,研究米氮平作为治疗多种IBS症状的潜在一站式治疗方法,其有可能减少多重用药和不良反应,尤其是在老年人群中。