Department of Cardiology, Faculty of Medicine, Slim Chaker University Hospital, University of Sfax, Sfax, Tunisia.
Department of Gynecology and Obstetrics, Faculty of Medicine, Hedi Chaker University Hospital, University of Sfax, Sfax, Tunisia.
BMC Pregnancy Childbirth. 2024 Nov 6;24(1):722. doi: 10.1186/s12884-024-06911-3.
Peripartum cardiomyopathy (PPCM) is a rare but potentially life-threatening condition. Due to the scarcity of epidemiological data in North Africa, we conducted this study to assess the outcomes of PPCM in our region.
This monocentric retrospective cohort study involving all patients diagnosed with PPCM was conducted between January 2010 and December 2022.
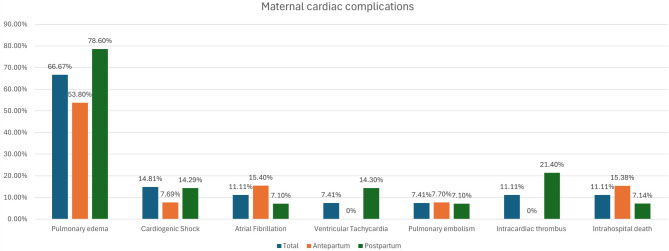
Twenty-seven PPCM patients, with a median age of 33 years (Interquartile range (IQR) = 9), were included. 52% of patients were diagnosed during the postpartum period. Dyspnea New York Heart Association III/IV(NYHA III/IV) was the most common functional symptom (85%). The median left ventricle ejection fraction (LVEF) was 30% (IQR = 11%). Atrial fibrillation occurred in 11.1% of patients, thromboembolic complications occurred in 18.5%, Pulmonary edema occurred in 85% of patients and cardiogenic shock occurred in 14.8% of patients, with two patients requiring Extracorporeal Membrane Oxygenation (ECMO) support. The predominant mode of delivery was a cesarean Sect. (82% of patients), and the indication for a cesarean delivery was obstetrical in 59% of patients. Prematurity occurred in 36% of newborns, and intrauterine fetal death occurred in one pregnancy. The median follow-up was 24 months [6-144 months]. LVEF recovery was noted in 67% of patients. Bromocriptine was administered to six patients (22%), and none of these patients died and out of them, five patients recovered their LVEF (83%). The overall mortality rate during the follow-up period was 15%, comprising three in-hospital cardiac deaths and one occurring two years later due to refractory advanced heart failure. No significant differences were observed between LVEF recovery and LVEF non-recovery groups. Factors significantly associated with mortality were multiparity, poor antenatal care (ANC) attendance, thromboembolic events, cardiogenic shock, and Pulmonary edema. Five patients with LV recovery subsequently became pregnant, none experienced a relapse of PPCM. However, one of the descendants of a patient was diagnosed with dilated cardiomyopathy.
This study revealed that the diagnosis of PPCM in our hospital is often delayed until symptoms become more advanced, resulting in high morbi-mortality.
围生期心肌病(PPCM)是一种罕见但潜在危及生命的疾病。由于北非缺乏流行病学数据,我们进行了这项研究,以评估我们地区 PPCM 的结局。
这是一项单中心回顾性队列研究,纳入了 2010 年 1 月至 2022 年 12 月期间所有诊断为 PPCM 的患者。
共纳入 27 例 PPCM 患者,中位年龄为 33 岁(四分位距[IQR] = 9)。52%的患者在产后期间被诊断。呼吸困难纽约心脏协会 III/IV 级(NYHA III/IV)是最常见的功能症状(85%)。左心室射血分数(LVEF)中位数为 30%(IQR = 11%)。11.1%的患者发生心房颤动,18.5%发生血栓栓塞并发症,85%的患者发生肺水肿,14.8%的患者发生心源性休克,其中 2 例需要体外膜肺氧合(ECMO)支持。主要的分娩方式为剖宫产(82%的患者),剖宫产的指征为产科原因的占 59%。新生儿早产发生率为 36%,1 例妊娠发生宫内胎儿死亡。中位随访时间为 24 个月[6-144 个月]。67%的患者 LVEF 恢复。6 例患者(22%)接受了溴隐亭治疗,这些患者均未死亡,其中 5 例患者的 LVEF 恢复(83%)。随访期间总死亡率为 15%,包括 3 例院内心源性死亡和 1 例 2 年后因难治性晚期心力衰竭死亡。LVEF 恢复组与 LVEF 未恢复组之间无显著差异。与死亡率显著相关的因素包括多胎妊娠、产前保健(ANC)不佳、血栓栓塞事件、心源性休克和肺水肿。5 例 LVEF 恢复的患者随后怀孕,均未复发 PPCM。然而,一名患者的后代被诊断为扩张型心肌病。
本研究表明,我院 PPCM 的诊断往往延迟至症状更为严重时才作出,导致高病死率。