Schmieder Roland E, Hettrick Douglas A, Böhm Michael, Kandzari David E, Kario Kazuomi, Mahfoud Felix, Tsioufis Konstantinos, Weber Michael A, Esler Murray D, Townsend Raymond R
University Hospital Erlangen, Erlangen, Germany.
Medtronic, Santa Rosa, CA, USA.
Hypertens Res. 2025 Jan;48(1):327-335. doi: 10.1038/s41440-024-01949-4. Epub 2024 Nov 14.
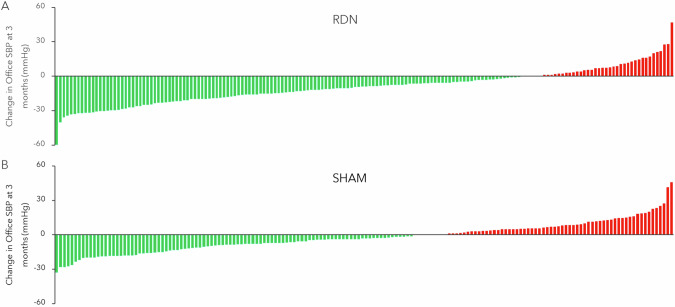
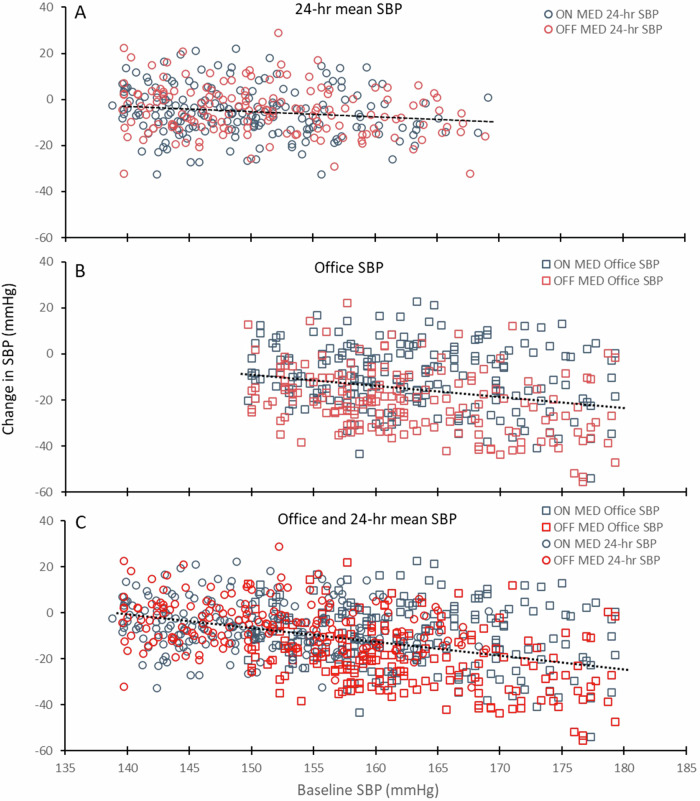
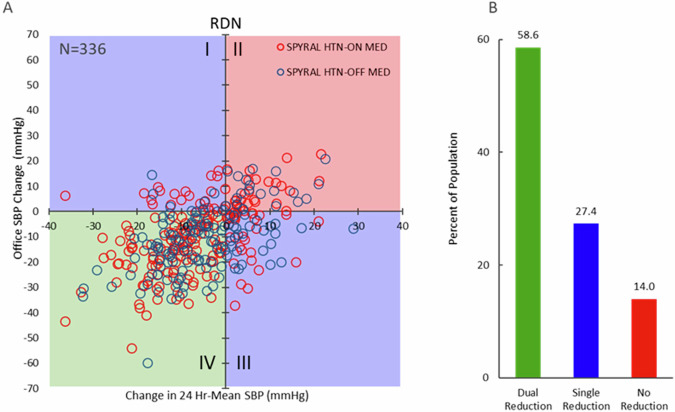
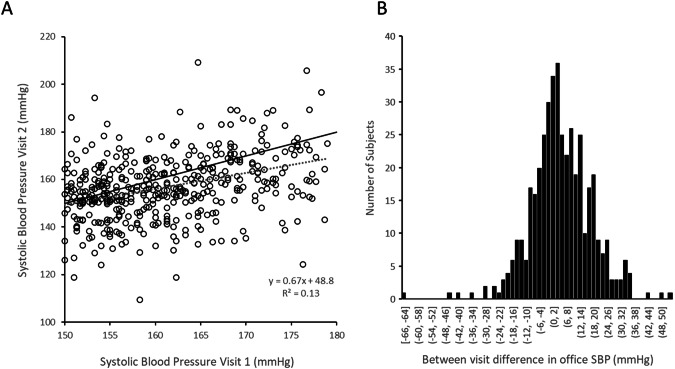
Multiple sham-controlled clinical trials have demonstrated significant reductions in both office and 24-h blood pressure (BP) following radiofrequency renal denervation (RDN) in the uncontrolled hypertension population. Notably, the blood pressure response varies widely within individual participants, thus showing a clinical need to identify potential RDN "responders" prior to the procedure. Despite multiple analytic efforts, no single parameter, aside from baseline blood pressure, has been consistently associated with BP reduction following RDN. However, this failure may be due to limitations in empiric definitions of responders. Indeed, commonly applied responder definitions based on the difference between two point-in-time BP measurements are fraught due to visit-to-visit variability in office and 24-h blood pressure endpoints. Several factors should be considered to develop a more clinically useful operational definition of procedural response including relative changes in office and 24-h BP, consideration of the temporal response to RDN, as well as adjustment for baseline BP. The current evidence may provide incentives for future expert consensus to precisely define responders to hypertension treatments.
多项假手术对照临床试验表明,在未控制的高血压人群中,经导管肾去交感神经术(RDN)后诊室血压和24小时血压(BP)均显著降低。值得注意的是,个体参与者的血压反应差异很大,因此表明在手术前有临床需求来识别潜在的RDN“反应者”。尽管进行了多项分析,但除了基线血压外,没有单一参数与RDN后的血压降低始终相关。然而,这种失败可能是由于反应者经验性定义的局限性。事实上,基于两个时间点血压测量值差异的常用反应者定义存在缺陷,因为诊室血压和24小时血压终点的就诊间变异性较大。为了制定更具临床实用性的手术反应操作定义,应考虑几个因素,包括诊室血压和24小时血压的相对变化、对RDN的时间反应以及对基线血压的调整。目前的证据可能会促使未来专家达成共识,以精确界定高血压治疗的反应者。