Andersen-Group, University of Southern Denmark, Campusvej 55, 5230, Odense, Denmark.
Department of Clinical Biochemistry, Odense University Hospital, Odense, Denmark.
Stem Cell Res Ther. 2024 Nov 14;15(1):426. doi: 10.1186/s13287-024-04037-z.
Injection of autologous adipose-derived regenerative cells (ADRCs) combined with lipotransfer has been suggested to alleviate symptoms in diseases including breast cancer-related lymphedema (BCRL). We recently performed a randomized controlled trial injecting lipoaspirate with ADRCs into the axilla of BCRL patients, and here we aimed in the intervention group to define in an unbiased fashion whether ADRC injection was linked to the clinical outcome.
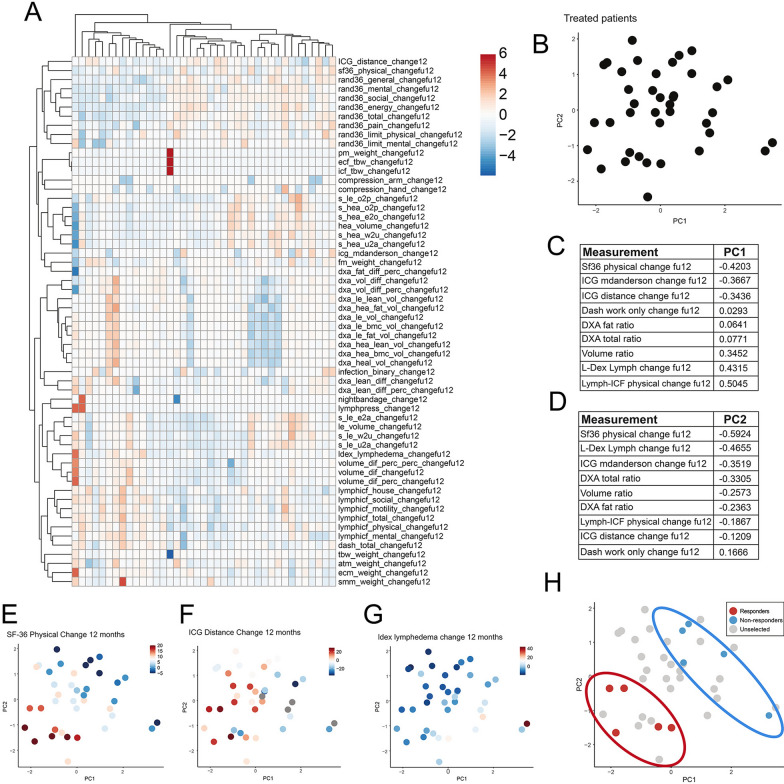
39 BCRL patients received lipotransfer assisted with autologous ADRCs (4.20 × 10 ± 1.75 × 10 cells) whereas 41 BCRL patients were included for placebo treatment. At 12 month follow-up, we assessed quality of life, lymphangiography, and bioimpedance enclosing 59 outcome parameters. Multifactorial analysis of clinical outcomes was used to define responders and non-responders to the intervention, and collected ADRCs from these patient groups were analyzed by single cell RNA sequencing (scRNAseq).
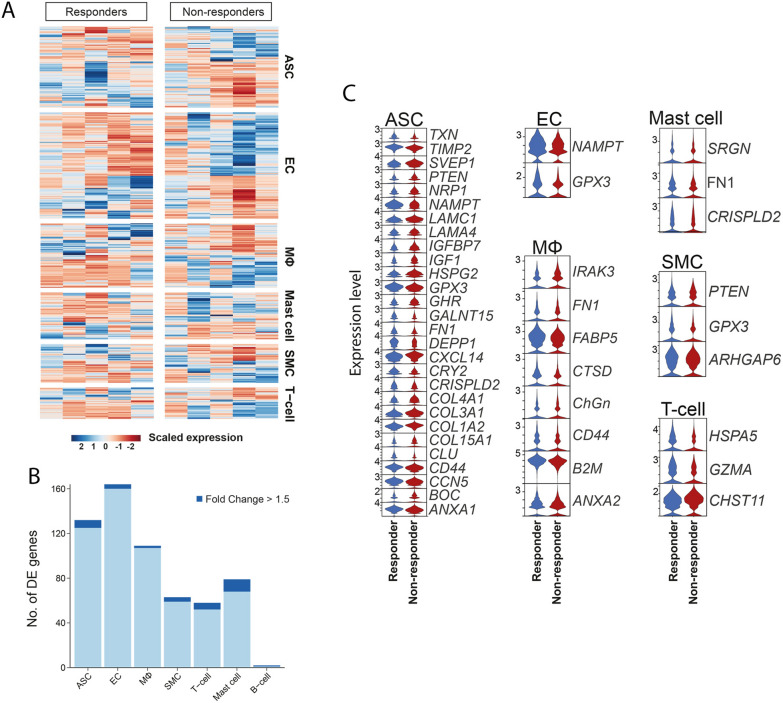
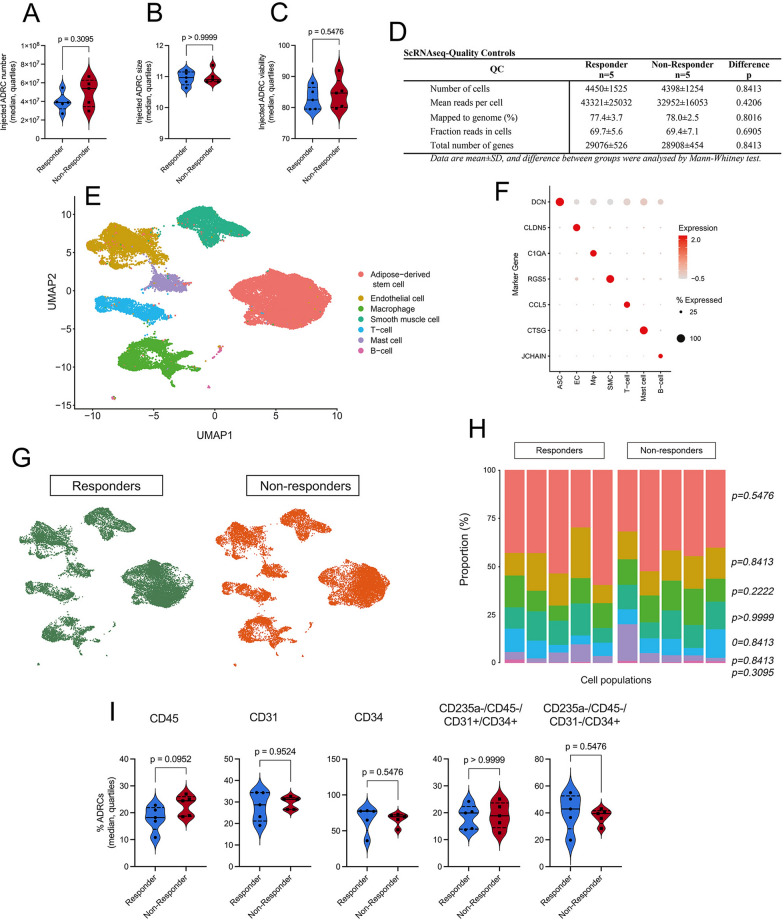
Unbiased multifactorial analysis ranked and defined the clinical outcomes (Sf36 physical change, L-Dex Lymph Change, ICG mdanderson change) with the highest effect on BCRL patients. The 10 patients with the highest- and lowest effect (five responders and five non-responders) were included in the study. No difference between non-responders and responders were observed for injected ADRC number/size/viability (p > 0.05). In scRNAseq, we did not find any major difference (p > 0.05) between groups in ADRC composition regarding adipose derived stem cells, endothelial-, smooth muscle-, T-, B-, mast cells as well as macrophages, which was verified by flow cytometry. Differential subcluster gene expression between groups were for 92.5% of genes, including those encoding secretory proteins, below the threshold of 1.5, and thus neglible. Together this suggested that the ADRC phenotype was indistinguishable between BCRL responders and non-responders to the intervention.
Our data suggest that the ADRC injection and ADRC phenotype or heterogeneity have no effect on the clinical outcomes on BCRL, and ADRC assisted lipotranfer for BCRL should therefore not be considered currently.
自体脂肪来源的再生细胞(ADRCs)注射与脂肪转移联合应用已被证明可缓解乳腺癌相关淋巴水肿(BCRL)等疾病的症状。我们最近对接受 BCRL 治疗的患者进行了一项随机对照试验,将脂肪抽吸物与 ADRC 注入腋窝,在此,我们旨在对干预组进行无偏倚的分析,以确定 ADRC 注射是否与临床结果相关。
39 例 BCRL 患者接受了自体 ADRC 辅助的脂肪转移(4.20×10±1.75×10 个细胞),而 41 例 BCRL 患者接受了安慰剂治疗。在 12 个月的随访中,我们评估了生活质量、淋巴造影术和包含 59 个结果参数的生物阻抗。采用多因素临床结果分析来定义对干预有反应和无反应的患者,并对这些患者组的 ADRC 进行单细胞 RNA 测序(scRNAseq)分析。
无偏倚的多因素分析对 BCRL 患者的临床结果(SF36 身体变化、L-Dex 淋巴变化、ICG mdanderson 变化)进行了排序和定义,其影响最大。将 10 名具有最高和最低影响的患者(5 名有反应者和 5 名无反应者)纳入研究。无反应者和有反应者之间注射的 ADRC 数量/大小/活力无差异(p>0.05)。在 scRNAseq 中,我们没有发现组间 ADRC 组成在脂肪来源干细胞、内皮细胞、平滑肌细胞、T 细胞、B 细胞、肥大细胞以及巨噬细胞方面有任何明显差异(p>0.05),这一结果通过流式细胞术得到了验证。组间差异亚群基因表达在 92.5%的基因中低于 1.5 的阈值,因此可以忽略不计。综上所述,这表明 ADRC 表型在 BCRL 对干预有反应者和无反应者之间没有区别。
我们的数据表明,ADRC 注射和 ADRC 表型或异质性对 BCRL 的临床结果没有影响,因此,目前不应考虑 ADRC 辅助脂肪转移治疗 BCRL。