Heuts Samuel, Kawczynski Michal J, Leus Arthur, Godinas Laurent, Belge Catharina, van Empel Vanessa, Meyns Bart, Maessen Jos G, Delcroix Marion, Verbelen Tom
Department of Cardiothoracic Surgery, Maastricht University Medical Centre (MUMC+), Maastricht, The Netherlands
Cardiovascular Research Institute Maastricht (CARIM), Maastricht University, Maastricht, The Netherlands.
Eur Respir J. 2025 Feb 27;65(2). doi: 10.1183/13993003.01865-2024. Print 2025 Feb.
We conducted a volume-outcome meta-analysis of pulmonary endarterectomy procedures for chronic thromboembolic pulmonary hypertension to objectively determine the minimum required annual case load that can define a high-volume centre.
Three electronic databases were systematically queried up to 1 May 2024. Centres were divided in volume tertiles. The primary outcomes were early mortality and long-term survival. Restricted cubic splines were used to demonstrate the volume-outcome relationship and the elbow-method was applied to define high-volume centres. Long-term survival was assessed using Cox frailty models.
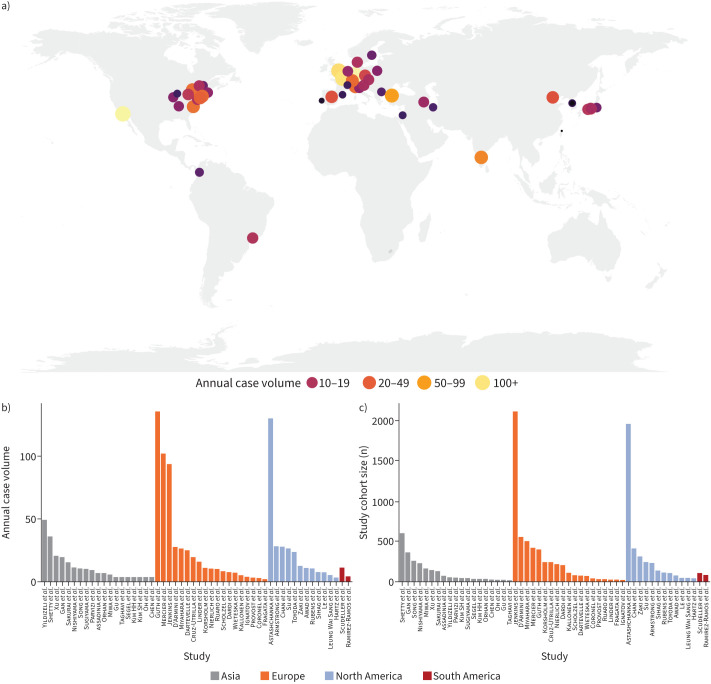
We included 51 centres (52 consecutive cohorts) and divided them into tertiles (T1: <6 cases per year; T2: 6-15 cases per year, T3: >15 cases per year), comprising a total 11 345 patients (mean age 52.3 years). Overall early mortality was 6.0% (T1: 11.6%; T2: 7.2%; T3: 5.2%; p<0.001), for which a significant nonlinear volume-outcome relationship was observed (p=0.0437) with a statistically determined minimal required volume of 33 cases per year (95% CI 29-35 cases), and a modelled volume of 40 cases per year corresponding to a 5.0% mortality rate. Nevertheless, early mortality still progressively declined in higher volume centres (from 6.7% to 5.4% to 2.9% in centres performing 16-50, 51-100 and >100 procedures annually). In addition, a significant volume effect was observed for long-term survival (adjusted hazard ratio per tertile 0.75, 95% CI 0.63-0.89; p=0.001).
There is a significant association between procedural volume and early mortality in pulmonary endarterectomy. An annual procedural volume of >33-40 cases per year may be used to define a high‑volume centre, although higher volumes still lead to progressively lower mortality rates.
我们对慢性血栓栓塞性肺动脉高压的肺动脉内膜剥脱术进行了一项容量-结局的荟萃分析,以客观确定能够定义高容量中心的最低年度病例数。
截至2024年5月1日,系统检索了三个电子数据库。将各中心分为三个容量三分位数组。主要结局为早期死亡率和长期生存率。使用受限立方样条来展示容量-结局关系,并应用折点法来定义高容量中心。使用Cox脆弱模型评估长期生存率。
我们纳入了51个中心(52个连续队列),并将它们分为三分位数组(T1:每年<6例;T2:每年6 - 15例;T3:每年>15例),共11345例患者(平均年龄52.3岁)。总体早期死亡率为6.0%(T1:11.6%;T2:7.2%;T3:5.2%;p<0.001),观察到显著的非线性容量-结局关系(p = 0.0437),经统计确定每年所需的最低病例数为33例(95%CI 29 - 35例),模型显示每年40例的病例数对应的死亡率为5.0%。然而,在更高容量的中心,早期死亡率仍在逐渐下降(每年进行16 - 50例、51 - 100例和>100例手术的中心,早期死亡率分别从6.7%降至5.4%再降至2.9%)。此外,观察到长期生存存在显著的容量效应(每三分位数组的调整风险比为0.75,95%CI 0.63 - 0.89;p = 0.001)。
肺动脉内膜剥脱术的手术量与早期死亡率之间存在显著关联。每年手术量>33 - 40例可用于定义高容量中心,尽管手术量越高,死亡率仍会逐渐降低。