Reeder Joshua A, Creech C Buddy, Nation Roger L, Gu Kenan, Nalbant Demet, Wu Nan, Jimenez-Truque Natalia, Fissell William, Rolsma Stephanie L, Fishbane Nicholas, Kirkpatrick Carl M J, Patel Pratish C, Watanabe Amy, Landersdorfer Cornelia B, Winokur Patricia, An Guohua
Department of Pharmaceutical Sciences and Experimental Therapeutics, College of Pharmacy, University of Iowa, Iowa City, IA, USA.
Division of Pediatric Infectious Diseases, Department of Pediatrics, Vanderbilt University Medical Center, Nashville, TN, USA.
J Clin Pharmacol. 2025 Apr;65(4):452-465. doi: 10.1002/jcph.6161. Epub 2024 Dec 3.
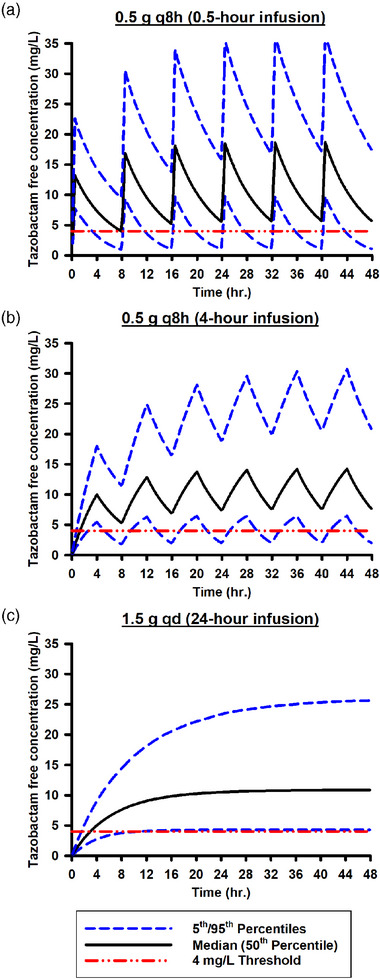
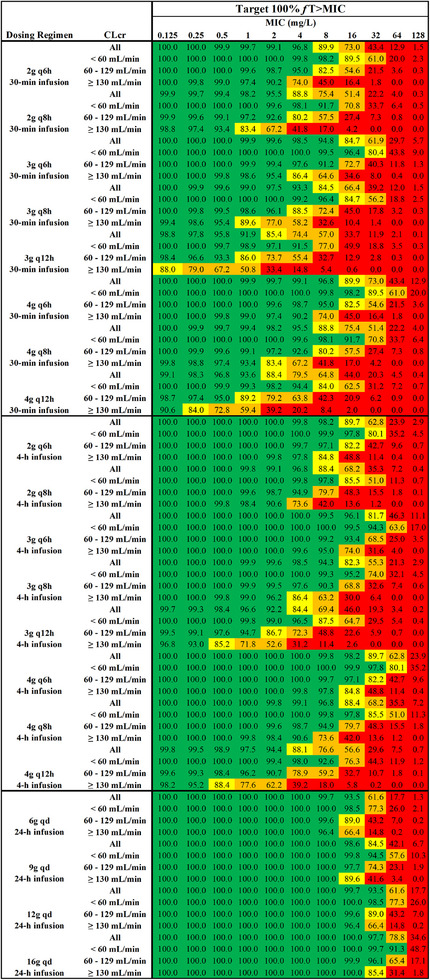
Determining an effective dosing regimen for piperacillin-tazobactam in critically ill patients is challenging due to substantial pharmacokinetic variability caused by complex pathophysiological changes. To address this need, a prospective clinical study was conducted, which enrolled 112 critically ill patients and employed an opportunistic sampling strategy. Population modeling and simulation were performed to characterize the pharmacokinetics (PK) and probability of target attainment (PTA) of piperacillin-tazobactam under various dosing regimens. Both piperacillin and tazobactam final models were one-compartment models with zero-order input and first-order elimination. Significant covariates included lean body weight for piperacillin and creatinine clearance along with continuous renal replacement therapy (CRRT) for both drugs. Monte Carlo simulations demonstrated that continuous infusion can achieve higher PTA than intermittent and extended infusions. When considering the minimum inhibitory concentration (MIC) of 16 mg/L for Pseudomonas aeruginosa (a frequently encountered bacterial pathogen among critically ill patients) and a PK/PD target of 100% fT >MIC, continuous infusion of 6 g/day is recommended for critically ill patients with a CLcr <60 mL/min, 9 g/day for patients with CLcr in the range of 60 to 129 mL/min, and 12 g/day for patients with a CLcr ≥130 mL/min. In addition, extended infusion represents a good alternative, especially the 3 g q6h or 4 g q6h regimens which can achieve the designated European Committee on Antimicrobial Susceptibility Testing (EUCAST) non-species-related PK/PD breakpoint of 8 mg/L. Our study provided valuable insight into PTA outcomes, which, together with individual renal function of future patients and institution-specific piperacillin susceptibility patterns, may assist physicians when making dosing decisions.
由于复杂的病理生理变化导致药代动力学存在显著差异,因此确定危重症患者哌拉西林-他唑巴坦的有效给药方案具有挑战性。为满足这一需求,开展了一项前瞻性临床研究,该研究纳入了112例危重症患者,并采用了机会性抽样策略。进行了群体建模和模拟,以表征不同给药方案下哌拉西林-他唑巴坦的药代动力学(PK)和达标概率(PTA)。哌拉西林和他唑巴坦的最终模型均为具有零级输入和一级消除的单室模型。显著的协变量包括哌拉西林的瘦体重、肌酐清除率以及两种药物的持续肾脏替代治疗(CRRT)。蒙特卡洛模拟表明,持续输注比间歇输注和延长输注能实现更高的PTA。当考虑铜绿假单胞菌(危重症患者中常见的细菌病原体)的最低抑菌浓度(MIC)为16 mg/L以及PK/PD目标为100% fT > MIC时,对于肌酐清除率(CLcr)<60 mL/min的危重症患者,建议持续输注6 g/天;CLcr在60至129 mL/min范围内的患者,9 g/天;CLcr≥130 mL/min的患者,12 g/天。此外,延长输注是一种很好的替代方案,尤其是3 g q6h或4 g q6h方案,其可达到欧洲抗菌药物敏感性试验委员会(EUCAST)指定的8 mg/L的非菌种相关PK/PD折点。我们的研究为PTA结果提供了有价值的见解,这与未来患者的个体肾功能以及机构特定的哌拉西林敏感性模式一起,可能有助于医生做出给药决策。