Dansero Lucia, Milani Lorenzo, Gnavi Roberto, Macciotta Alessandra, Destefanis Cinzia, Gilcrease Winston, Sciascia Savino, Ricceri Fulvio
Centre for Biostatistics, Epidemiology, and Public Health, Department of Clinical and Biological Sciences, University of Turin, Orbassano (TO), Italy
Centre for Biostatistics, Epidemiology, and Public Health, Department of Clinical and Biological Sciences, University of Turin, Orbassano (TO), Italy.
J Epidemiol Community Health. 2025 Apr 10;79(5):366-372. doi: 10.1136/jech-2024-222370.
Chronic kidney disease (CKD) and end-stage renal disease (ESRD) represent significant public health challenges, linked to an elevated risk of cardiovascular disease (CVD) and influenced by socioeconomic disparities. This longitudinal study investigates the interplay between socioeconomic position (SEP), measured as educational level, CKD/ESRD and CVD using the syndemic framework.
We used data from the Piedmont Longitudinal Study to establish CKD and ESRD cohorts and to identify incident CVD between January 2013 and December 2017. The educational level was retrieved from census data. We applied an accelerated failure time model to explore the relationships between CKD/ESRD, CVD and educational level with all-cause mortality and emergency room (ER) acuity.
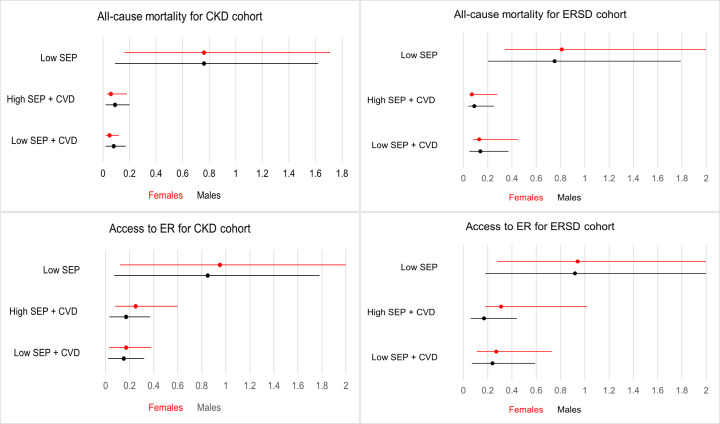
The CKD cohort included 44 220 individuals, with 12 341 deaths and 15 440 ER admissions. The ESRD cohort included 4021 subjects, experiencing 1303 deaths and 1640 ER admissions. After adjusting for confounders, the combination of CKD, low educational level and incident CVD was associated with increased all-cause mortality (time ratios (TR) 0.07, 95% CI 0.05 to 0.08) and ER acuity (TR 0.16, 95% CI 0.14 to 0.17) compared with those with higher education. Instead, patients with ESRD with incident CVD and high educational level had the highest increase in mortality (TR 0.08, 95% CI 0.05 to 0.14) and ER acuity (TR 0.20, 95% CI 0.1 to 0.30).
Patients with CKD with low educational levels and incident CVD may represent a 'syndemic', associated with higher mortality and ER acuity. Our study highlights a potential link between these conditions and socioeconomic disparities, suggesting the need for multifaceted approaches.
慢性肾脏病(CKD)和终末期肾病(ESRD)是重大的公共卫生挑战,与心血管疾病(CVD)风险升高相关,并受到社会经济差异的影响。这项纵向研究使用综合征框架调查了以教育水平衡量的社会经济地位(SEP)、CKD/ESRD和CVD之间的相互作用。
我们使用皮埃蒙特纵向研究的数据来建立CKD和ESRD队列,并确定2013年1月至2017年12月期间的新发CVD。教育水平从人口普查数据中获取。我们应用加速失效时间模型来探讨CKD/ESRD、CVD和教育水平与全因死亡率和急诊室(ER)急症之间的关系。
CKD队列包括44220人,其中12341人死亡,15440人入院接受急诊治疗。ESRD队列包括4021名受试者,其中1303人死亡,1640人入院接受急诊治疗。在调整混杂因素后,与受过高等教育的人相比,CKD、低教育水平和新发CVD的组合与全因死亡率增加(时间比(TR)0.07,95%CI 0.05至0.08)和ER急症(TR 0.16,95%CI 0.14至0.17)相关。相反,患有新发CVD且教育水平高的ESRD患者死亡率(TR 0.08,95%CI从0.05至0.14)和ER急症(TR 0.20,95%CI 0.1至0.30)的增加幅度最大。
教育水平低且患有新发CVD的CKD患者可能代表一种“综合征”,与更高的死亡率和ER急症相关。我们的研究强调了这些情况与社会经济差异之间的潜在联系,表明需要采取多方面的方法。