Meng He, Zhou Xiujun, Li Lushan, Liu Yuanying, Liu Yujie, Zhang Ying
Department of Cardiology, Tianjin Chest Hospital, No.261 of Taierzhuangnan Road, Jinnan District, Tianjin, 300222, People's Republic of China.
Department of Cardiology, Chest Hospital, Tianjin University, No.261 of Taierzhuangnan Road, Jinnan District, Tianjin, 300222, People's Republic of China.
Sci Rep. 2024 Dec 4;14(1):30175. doi: 10.1038/s41598-024-81818-9.
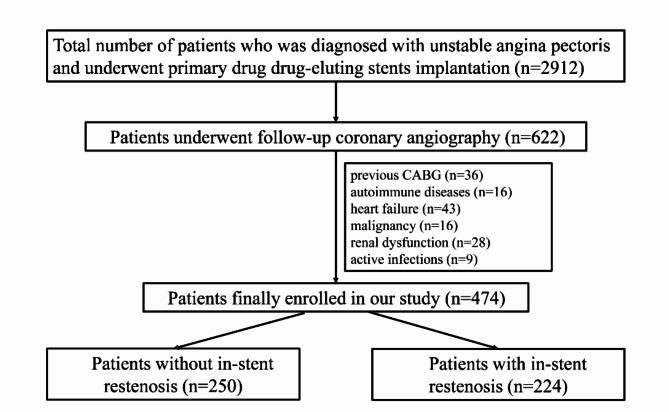
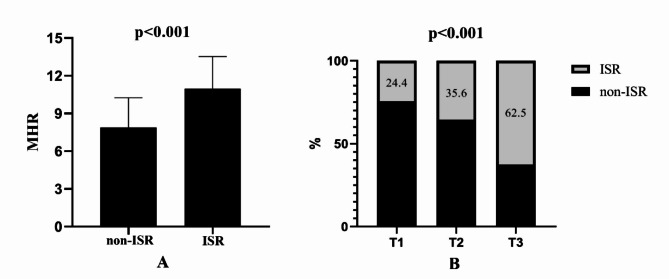
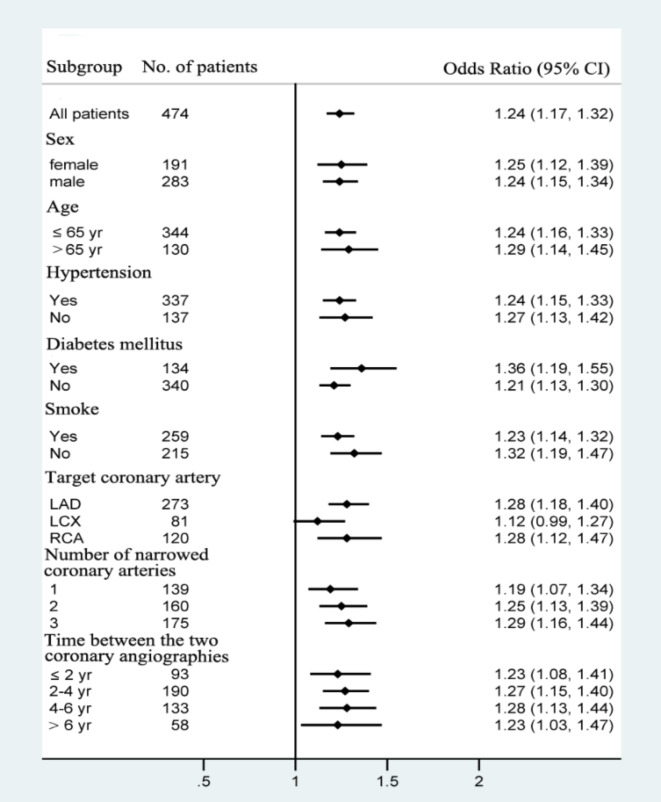
Several studies have shown that the monocyte count to high-density lipoprotein cholesterol ratio (MHR) serves as a predictive marker for in-stent restenosis (ISR) of bare-metal stents (BMSs). However, the ability of the MHR to predict ISR in patients with drug-eluting stents (DESs) remains uncertain. This study aimed to investigate the predictive value of the MHR for ISR in patients with unstable angina pectoris who have undergone primary DES implantation. A total of 474 consecutive patients with unstable angina pectoris who underwent successful DES-based percutaneous coronary intervention (PCI) from 01-12-2014 to 01-12-2022 were enrolled in the study. Patients were divided into the ISR group and the non-ISR group on the basis of the follow-up results of coronary angiography. The demographic and clinical characteristics of the patients were documented. The MHR was calculated via the following formula: [Formula: see text]. Multivariate logistic regression models were developed to evaluate the predictive value of the MHR for DES-ISR. The baseline MHR was notably greater in the ISR group than in the non-ISR group (P < 0.001). After adjusting for confounding factors, the MHR emerged as an independent predictor of ISR (OR = 1.244; 95%CI 1.171-1.321). Receiver operating characteristic (ROC) curve analysis revealed that MHR for predicting ISR had an AUC of 0.752 (95% CI 0.708-0.796). For a MHR > 7.32, the sensitivity was estimated to be 59.8% (95% CI 47.2-66.5%) and the specificity was 81.2% (95% CI 71.2-86.4%). Including the MHR in the predictive model for ISR improved the area under the curve (0.698 vs. 0.782, P < 0.001), categorical net reclassification improvement (0.703; 95%CI 0.536-0.871), and integrated discrimination improvement (0.121; 95%CI 0.092-0.151). The MHR can be used to predict DES-ISR in patients with unstable angina pectoris, indicating that the MHR may serve as a valuable marker for risk stratification and prognosis in individuals undergoing DES implantation.
多项研究表明,单核细胞计数与高密度脂蛋白胆固醇比值(MHR)可作为裸金属支架(BMS)支架内再狭窄(ISR)的预测指标。然而,MHR对药物洗脱支架(DES)患者ISR的预测能力仍不确定。本研究旨在探讨MHR对接受初次DES植入的不稳定型心绞痛患者ISR的预测价值。本研究纳入了2014年12月1日至2022年12月1日期间连续474例成功接受基于DES的经皮冠状动脉介入治疗(PCI)的不稳定型心绞痛患者。根据冠状动脉造影的随访结果,将患者分为ISR组和非ISR组。记录患者的人口统计学和临床特征。MHR通过以下公式计算:[公式:见正文]。建立多因素逻辑回归模型以评估MHR对DES-ISR的预测价值。ISR组的基线MHR显著高于非ISR组(P<0.001)。在调整混杂因素后,MHR成为ISR的独立预测因子(OR=1.244;95%CI 1.171-1.321)。受试者工作特征(ROC)曲线分析显示,用于预测ISR的MHR的AUC为0.752(95%CI 0.708-0.796)。对于MHR>7.32,估计敏感性为59.8%(95%CI 47.2-66.5%),特异性为81.2%(95%CI 71.2-86.4%)。将MHR纳入ISR预测模型可改善曲线下面积(0.698对0.782;P<0.001)、分类净重新分类改善(0.703;95%CI 0.536-0.8