Tabbara Nadeem, Dioverti-Prono M Veronica, Jain Tania
Johns Hopkins Sidney Kimmel Comprehensive Cancer Center, Baltimore, MD.
Division of Infectious Disease, Department of Medicine, Johns Hopkins School of Medicine, Baltimore, MD.
Hematology Am Soc Hematol Educ Program. 2024 Dec 6;2024(1):116-125. doi: 10.1182/hematology.2024000535.
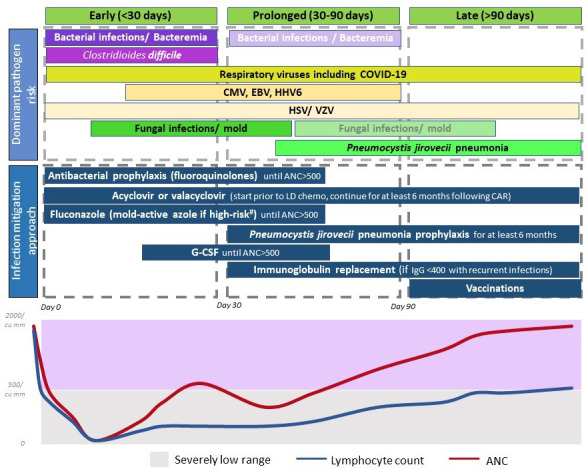
Chimeric antigen receptor T-cell therapy (CAR-T) has transformed the treatment paradigm of relapsed/refractory B-cell malignancies. Yet, this therapy is not without toxicities. While the early inflammation-mediated toxicities are now better understood, delayed hematopoietic recovery and infections result in morbidity and mortality risks that persist for months following CAR-T. The predisposition to infections is a consequence of immunosuppression from the underlying disease, prior therapies, lymphodepletion chemotherapy, delayed hematopoietic recovery, B-cell aplasia, and delayed T-cell immune reconstitution. These risks and epidemiology can vary over a post-CAR-T timeline of early (<30 days), prolonged (30-90 days), or late (>90 days) follow-up. Antibacterial, antiviral, and antifungal prophylaxis; growth factors and stem cell boost to expedite count recovery; immunoglobulin replacement therapy; and possibly revaccination programs are important prevention strategies to consider for infection mitigation. Assessment of risk factors, evaluation, and treatment for pathogen(s) prevalent in a particular time frame post-CAR-T are important clinical considerations in patients presenting with clinical features suggestive of infectious pathology. As more data emerge on the topic, personalized risk assessments to inform the type and duration of prophylaxis use and planning interventions will continue to emerge. Herein, we review our current approach toward infection mitigation while recognizing that this continues to evolve and that there are differences among practices stemming from data availability limitations.
嵌合抗原受体T细胞疗法(CAR-T)已经改变了复发/难治性B细胞恶性肿瘤的治疗模式。然而,这种疗法并非没有毒性。虽然早期炎症介导的毒性现在已得到更好的理解,但延迟的造血恢复和感染会导致发病率和死亡风险,这些风险在CAR-T治疗后的数月内持续存在。易发生感染是由基础疾病、先前的治疗、淋巴细胞清除化疗、延迟的造血恢复、B细胞发育不全以及延迟的T细胞免疫重建导致的免疫抑制所造成的结果。这些风险和流行病学情况在CAR-T治疗后的早期(<30天)、延长(30 - 90天)或晚期(>90天)随访时间线上可能会有所不同。抗菌、抗病毒和抗真菌预防;使用生长因子和促进干细胞以加快血细胞计数恢复;免疫球蛋白替代疗法;以及可能的重新接种疫苗计划是减轻感染需要考虑的重要预防策略。评估CAR-T治疗后特定时间段内流行病原体的风险因素、进行评估及治疗,是对具有提示感染性病理临床特征的患者进行临床考虑的重要方面。随着关于该主题的更多数据出现,用于指导预防措施类型和持续时间以及规划干预措施的个性化风险评估将不断涌现。在此,我们回顾我们目前减轻感染的方法,同时认识到这仍在不断发展,并且由于数据可用性限制,不同实践之间存在差异。