Maylin Zoe R, Smith Christopher, Classen Adam, Asim Mohammad, Pandha Hardev, Wang Yuzhuo
Vancouver Prostate Centre, Department of Urological Sciences, University of British Columbia, Vancouver, BC V6H 3Z6, Canada.
Department of Experimental Therapeutics, BC Cancer Agency, Vancouver, BC V5Z 4E6, Canada.
Cells. 2024 Dec 3;13(23):1999. doi: 10.3390/cells13231999.
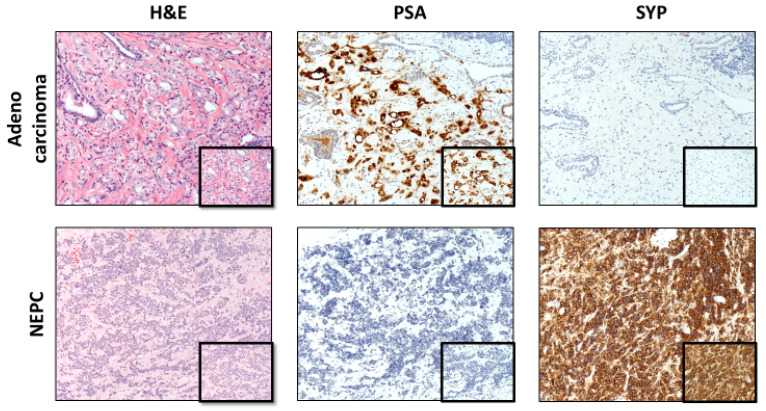
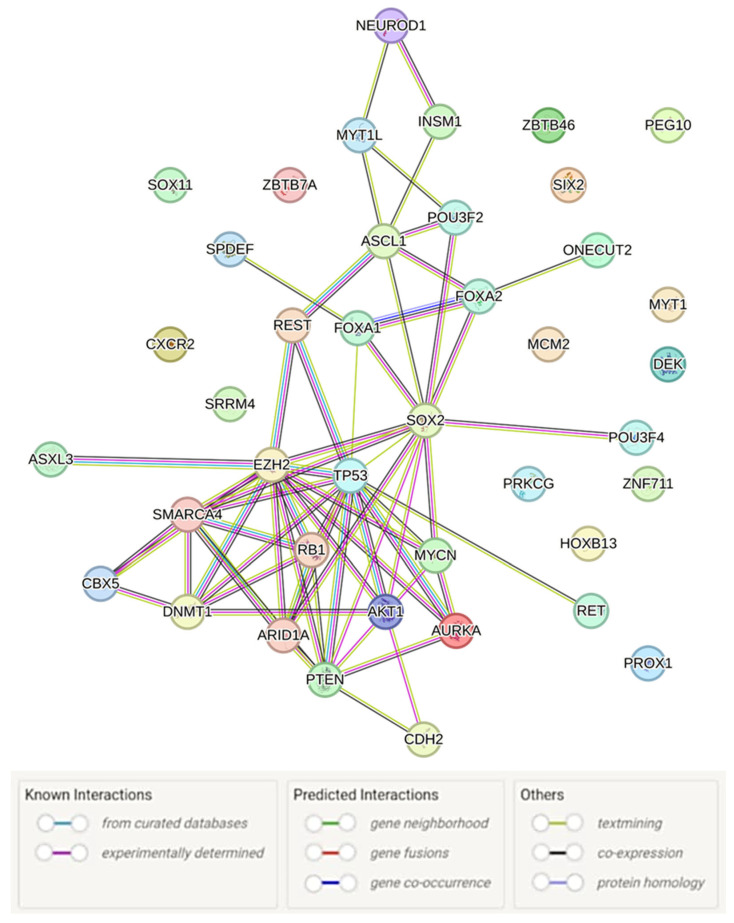
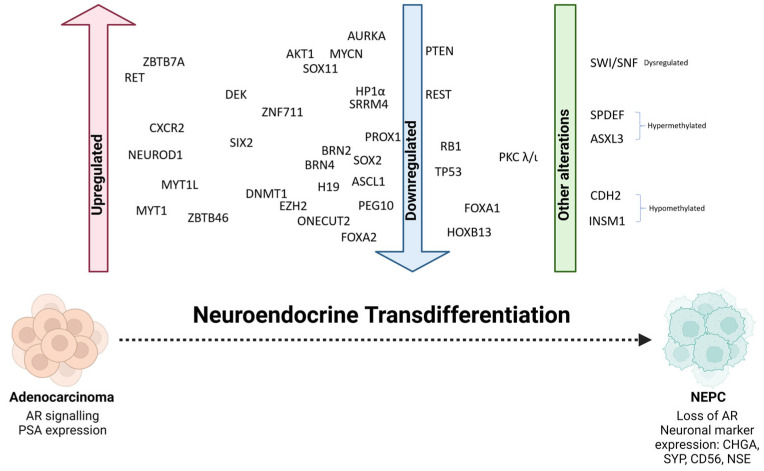
Neuroendocrine prostate cancer (NEPC), an aggressive and lethal subtype of prostate cancer (PCa), often arises as a resistance mechanism in patients undergoing hormone therapy for prostate adenocarcinoma. NEPC is associated with a significantly poor prognosis and shorter overall survival compared to conventional prostate adenocarcinoma due to its aggressive nature and limited response to standard of care therapies. This transdifferentiation, or lineage reprogramming, to NEPC is characterised by the loss of androgen receptor (AR) and prostate-specific antigen (PSA) expression, and the upregulation of neuroendocrine (NE) biomarkers such as neuron-specific enolase (NSE), chromogranin-A (CHGA), synaptophysin (SYP), and neural cell adhesion molecule 1 (NCAM1/CD56), which are critical for NEPC diagnosis. The loss of AR expression culminates in resistance to standard of care PCa therapies, such as androgen-deprivation therapy (ADT) which target the AR signalling axis. This review explores the drivers of NE transdifferentiation. Key genetic alterations, including those in the tumour suppressor genes RB1, TP53, and PTEN, and changes in epigenetic regulators, particularly involving EZH2 and cell-fate-determining transcription factors (TFs) such as SOX2, play significant roles in promoting NE transdifferentiation and facilitate the lineage switch from prostate adenocarcinoma to NEPC. The recent identification of several other key novel drivers of NE transdifferentiation, including MYCN, ASCL1, BRN2, ONECUT2, and FOXA2, further elucidates the complex regulatory networks and pathways involved in this process. We suggest that, given the multifactorial nature of NEPC, novel therapeutic strategies that combine multiple modalities are essential to overcome therapeutic resistance and improve patient outcomes.
神经内分泌前列腺癌(NEPC)是前列腺癌(PCa)的一种侵袭性致死亚型,常作为前列腺腺癌患者接受激素治疗时的一种耐药机制出现。与传统前列腺腺癌相比,NEPC预后明显较差,总生存期较短,这是由于其侵袭性本质以及对标准治疗方案反应有限。这种向NEPC的转分化或谱系重编程的特征是雄激素受体(AR)和前列腺特异性抗原(PSA)表达丧失,以及神经内分泌(NE)生物标志物如神经元特异性烯醇化酶(NSE)、嗜铬粒蛋白A(CHGA)、突触素(SYP)和神经细胞黏附分子1(NCAM1/CD56)上调,这些生物标志物对NEPC诊断至关重要。AR表达丧失最终导致对标准的PCa治疗方案耐药,如针对AR信号轴的雄激素剥夺疗法(ADT)。本综述探讨了NE转分化的驱动因素。关键的基因改变,包括肿瘤抑制基因RB1、TP53和PTEN中的改变,以及表观遗传调节因子的变化,特别是涉及EZH2和细胞命运决定转录因子(TFs)如SOX2的变化,在促进NE转分化和推动从前列腺腺癌到NEPC的谱系转换中起重要作用。最近发现的其他几个NE转分化的关键新驱动因素,包括MYCN、ASCL1、BRN2、ONECUT2和FOXA2,进一步阐明了这一过程中涉及的复杂调控网络和途径。我们认为,鉴于NEPC的多因素性质,结合多种方式的新型治疗策略对于克服治疗耐药性和改善患者预后至关重要。