Ferrara Gaetano, Nasuto Michelangelo, Napolitano Francesco, Ciccarese Giovanni, Aucella Filippo
Nephrology and Dialysis Unit, IRCCS Casa Sollievo Della Sofferenza Hospital, 71013 San Giovanni Rotondo, Italy.
Department of Radiological Sciences, Fondazione IRCCS Casa Sollievo Della Sofferenza, 71013 San Giovanni Rotondo, Italy.
J Clin Med. 2024 Dec 1;13(23):7307. doi: 10.3390/jcm13237307.
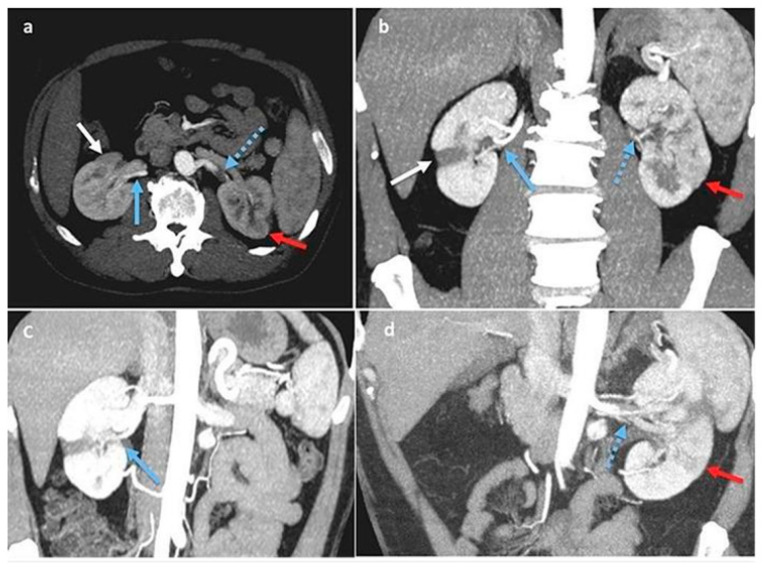
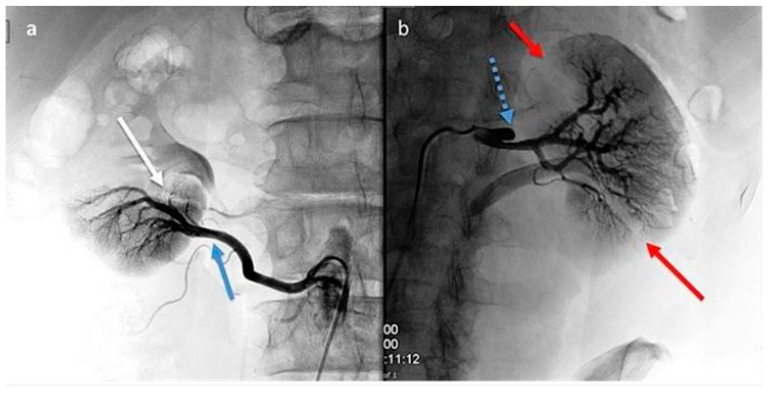
As spontaneous renal artery dissection (SRAD) is a rare cause of abdominal pain, bilateral dissection is an extremely rare event. Only approximately two hundred cases of SRAD have been reported in the literature. The diagnosis is often delayed due to the rarity of the disease and non-specific clinical presentations such as flank pain, hypertension, fever, nausea, vomiting, and hematuria, which can be often misdiagnosed as a genito-urinary infection or gastrointestinal or bowel disease. Before 1980, the diagnosis of SRAD was mostly confirmed via autopsy or, rarely, via angiography. At present, the diagnosis is made using advanced imaging approaches, including computed tomography angiography (CTA) and magnetic resonance angiography (MRA), with a higher number of incidentally diagnosed SRADs. we performed laboratory tests and radiological examinations (computed abdominal tomography and multiplanar reconstruction) that revealed multiple infarctions and ischemic areas with hypoperfusion in the upper middle third of the left kidney and in a large part of middle and lower areas of the right kidney; the left renal artery exhibited increased intimal thickening and arteritis. The multiplanar reconstruction revealed bilateral renal artery dissection and multiple arterial infarctions disseminated throughout both kidneys. After a clinical follow-up and hypertension retargeting, the patient was discharged with dual antiplatelet therapy and ACE inhibitor drugs. No lipid-lowering therapy was needed. Spontaneous renal artery dissection (SRAD) is a rare clinical event that typically presents with acute low-back or flank pain, hypertension, fever, hematuria, and acute renal failure. The condition could be misdiagnosed or receive a delayed diagnosis due to its relative rarity and non-specific presentation. The gold standard is enhanced computed tomography (CT) scans, and if the diagnosis is positive, vascular multiplanar reconstruction is generally suggested, as it can display lesions more clearly. Over 300 cases have been reported since the first characterization of SRAD; however, to date, a consensus has not been reached on the most appropriate treatment. Conservative therapy, open surgery, and intravascular intervention have been reported as treatments for SRAD.
由于自发性肾动脉夹层(SRAD)是腹痛的罕见原因,双侧夹层更是极为罕见的情况。文献中仅报道了约200例SRAD病例。由于该疾病罕见且临床表现不具特异性,如胁腹痛、高血压、发热、恶心、呕吐和血尿等,这些症状常被误诊为泌尿生殖系统感染或胃肠道疾病,导致诊断往往延迟。1980年以前,SRAD的诊断大多通过尸检确认,很少通过血管造影确诊。目前,诊断采用先进的成像方法,包括计算机断层血管造影(CTA)和磁共振血管造影(MRA),偶然诊断出的SRAD病例数量有所增加。我们进行了实验室检查和放射学检查(腹部计算机断层扫描和多平面重建),结果显示左肾中上三分之一以及右肾中下部大部分区域存在多处梗死和缺血区域以及灌注不足;左肾动脉内膜增厚和动脉炎加重。多平面重建显示双侧肾动脉夹层和遍布双肾的多处动脉梗死。经过临床随访和高血压重新调整治疗目标后,患者接受双联抗血小板治疗和ACE抑制剂药物后出院。无需降脂治疗。自发性肾动脉夹层(SRAD)是一种罕见的临床事件,通常表现为急性腰背痛或胁腹痛、高血压、发热、血尿和急性肾衰竭。由于其相对罕见和非特异性表现,该病可能被误诊或诊断延迟。金标准是增强计算机断层扫描(CT),如果诊断为阳性,一般建议进行血管多平面重建,因为它能更清晰地显示病变。自首次描述SRAD以来,已报道了300多例病例;然而,迄今为止,对于最合适的治疗方法尚未达成共识。保守治疗、开放手术和血管内介入已被报道为SRAD的治疗方法。