Taplin Katherine, Hannan Raquibul, Lo Simon S, Morgan Scott C, Ali Muhammad, Sigurdson Samantha, Guckenberger Matthias, Swaminath Anand
Faculty of Health Sciences, McMaster University, Hamilton, ON, Canada.
University of Texas - Southwestern Medical Center, Dallas, TX, USA.
Clin Transl Radiat Oncol. 2024 Nov 21;50:100891. doi: 10.1016/j.ctro.2024.100891. eCollection 2025 Jan.
To conduct an international survey of radiation oncologists treating primary renal cell carcinoma (RCC) with SABR to ascertain the general patterns of SABR use, common dose/treatment/follow-up details, and expected outcomes.
A 51-question survey was created containing the following themes: prevalence and clinical scenarios in which RCC SABR is used, dose-fractionation schedules, treatment delivery details, follow-up/outcome assessments, and implementation barriers. The survey was distributed widely across multiple influential radiation oncology societies and social media, and ran from January to April 2023.
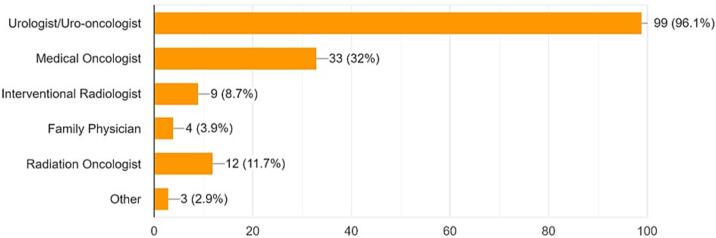
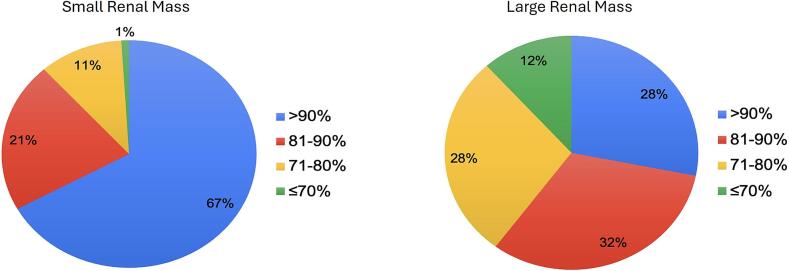
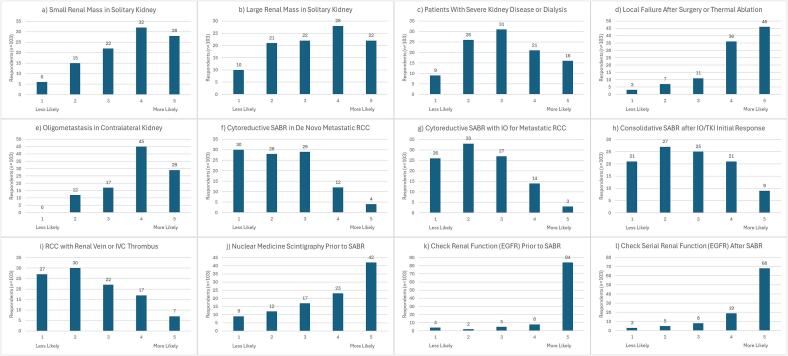
A total of 255 respondents participated, mostly from academic centers within Europe/North America. Of these, 40 % (n = 102) currently offer SABR (50 % having begun within the last 3 years). Common barriers in non-users included lack of referrals by urologists and lack of supportive practice guidelines. Of respondents who do offer SABR, 77 % treat both small (4 cm or less) and large (>4 cm) renal masses. Dose-fractionation strategies varied from 27-52 Gy (3-5 fractions) for multifraction regimens, and 15-34 Gy for single fractions. Apart from treatment for medically inoperable disease, scenarios in which SABR was likely to be offered were for recurrence post surgery/thermal ablation and for oligometastatic kidney lesions. Uncommon scenarios included RCC with renal vein/inferior vena cava thrombosis, and as cytoreductive therapy in metastatic RCC. Expected local control outcomes were generally above 70 %, higher for small versus large renal masses.
SABR is a relatively newer indication for primary RCC, offered by less than 50% of respondents, with both consistent and variable practice patterns observed.
对采用立体定向体部放疗(SABR)治疗原发性肾细胞癌(RCC)的放射肿瘤学家进行一项国际调查,以确定SABR的使用总体模式、常见的剂量/治疗/随访细节以及预期结果。
设计了一份包含51个问题的调查问卷,涵盖以下主题:RCC-SABR的使用患病率和临床场景、剂量分割方案、治疗实施细节、随访/结果评估以及实施障碍。该调查于2023年1月至4月在多个有影响力的放射肿瘤学会和社交媒体上广泛分发。
共有255名受访者参与,大多数来自欧洲/北美的学术中心。其中,40%(n = 102)目前提供SABR(50%在过去3年内开始提供)。未使用者的常见障碍包括泌尿科医生转诊不足和缺乏支持性的实践指南。在提供SABR的受访者中,77%治疗小(4 cm或更小)和大(>4 cm)肾肿块。多分割方案的剂量分割策略从27 - 52 Gy(3 - 5次分割)不等,单次分割为15 - 34 Gy。除了治疗医学上无法手术的疾病外,可能提供SABR的场景包括手术后/热消融后的复发以及寡转移肾病变。不常见的场景包括伴有肾静脉/下腔静脉血栓形成的RCC,以及作为转移性RCC的细胞减灭治疗。预期的局部控制率通常高于70%,小肾肿块高于大肾肿块。
SABR是原发性RCC相对较新的适应证,不到50%的受访者提供该治疗,观察到既有一致的也有可变的实践模式。