Haddad Sara, Dee Kevin, Chiang Augusto Dulanto, Feller Fionna, Ding Tan, Ayers Gregory D, Potts Marissa, LaRue Richard W
Department of Medicine, Division of Infectious Diseases, Vanderbilt University Medical Center, Nashville, Tennessee, USA.
Department of Biostatistics, Vanderbilt University Medical Center, Nashville, Tennessee, USA.
Transpl Infect Dis. 2025 Mar-Apr;27(2):e14418. doi: 10.1111/tid.14418. Epub 2024 Dec 18.
Cytomegalovirus (CMV) disease causes significant morbidity among solid organ transplant (SOT) recipients. To prevent CMV disease, eligible recipients are frequently started on valganciclovir (VGC) prophylaxis post-transplant. Leukopenia has been documented as a primary adverse events of the drug (1). This study's primary aim was to determine whether a patient's weight at the start of VGC prophylaxis was associated with the development of leukopenia.
This was a single center, retrospective cohort study that included adults > 18 years of age, who had received an organ transplant (heart, liver, or lung) at an academic transplant center from January 1, 2018 through December 31, 2022. A creatinine clearance of > 60 mL/min was required.
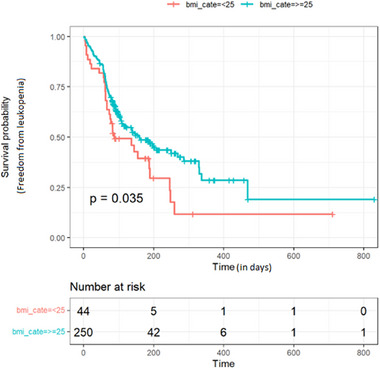
All 294 included patients received 900 mg/day of VGC for CMV prophylaxis, without dose adjustment. Fifty-two percent of the patients developed leukopenia while receiving VGC prophylaxis. The mean weight at initiation of VGC was higher in patients who did not develop leukopenia (97.9 kg) compared to those who did (90.7 kg; p = 0.0112). It was found that with each 1 kg increase in body weight, the likelihood of developing leukopenia decreased by 1.7% (p = 0.004, odds ratio = 0.983, 95% confidence interval [CI], 0.972-0.994). Patients with a baseline body-mass index (BMI) > 25 had a longer median freedom time from leukopenia after initiation of VGC as compared to the group with baseline BMI < 25 (log-rank p = 0.035).
These data suggest that in SOT recipients with normal renal function, receiving a fixed dose of VGC resulted in a significant, inverse relationship between body weight and the development of leukopenia.
巨细胞病毒(CMV)疾病在实体器官移植(SOT)受者中导致显著的发病情况。为预防CMV疾病,符合条件的受者在移植后常开始接受缬更昔洛韦(VGC)预防治疗。白细胞减少已被记录为该药物的主要不良事件(1)。本研究的主要目的是确定VGC预防治疗开始时患者的体重是否与白细胞减少的发生有关。
这是一项单中心回顾性队列研究,纳入了2018年1月1日至2022年12月31日在一家学术移植中心接受器官移植(心脏、肝脏或肺)的18岁以上成年人。要求肌酐清除率>60 mL/min。
所有294例纳入患者均接受900 mg/天的VGC进行CMV预防,未进行剂量调整。52%的患者在接受VGC预防治疗时出现白细胞减少。未发生白细胞减少的患者开始使用VGC时的平均体重(97.9 kg)高于发生白细胞减少的患者(90.7 kg;p = 0.0112)。研究发现,体重每增加1 kg,发生白细胞减少的可能性降低1.7%(p = 0.004,比值比 = 0.983,95%置信区间[CI],0.972 - 0.994)。与基线体重指数(BMI)<25的组相比,基线BMI>25的患者在开始使用VGC后白细胞减少的中位无事件时间更长(对数秩检验p = 0.035)。
这些数据表明,在肾功能正常的SOT受者中,接受固定剂量的VGC会导致体重与白细胞减少的发生之间存在显著的负相关关系。