Zhu Wenjiao, Lai Zhiman, Xue Miaorong, Feng Shaozhen, Feng Pinning, Pan Xiantian, Ke Xiaojie, Chen Xionghui, Li Zhijian, Mao Haiping, Yang Xiao, Huang Fengxian, Chen Wei, Xu Yuanwen, Li Shurong, Guo Qunying
Department of Nephrology, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, China.
NHC Key Laboratory of Clinical Nephrology (Sun Yat-Sen University) and Guangdong Provincial Key Laboratory of Nephrology, Guangzhou, China.
Ren Fail. 2025 Dec;47(1):2440512. doi: 10.1080/0886022X.2024.2440512. Epub 2024 Dec 18.
Vascular calcification (VC), especially coronary artery calcification (CAC), serves as a robust predictor of cardiovascular mortality in chronic kidney disease (CKD) patients. Recent studies have revealed that the presence of extra-coronary calcifications (ECCs) contributes to cardiovascular disease (CVD). Elevated myocardial injury markers predict mortality risk in CKD patients and are associated with CVD. Nevertheless, the relationship between VC, including CAC and ECCs, and myocardial injury markers remain unexplored in non-dialysis CKD patients.
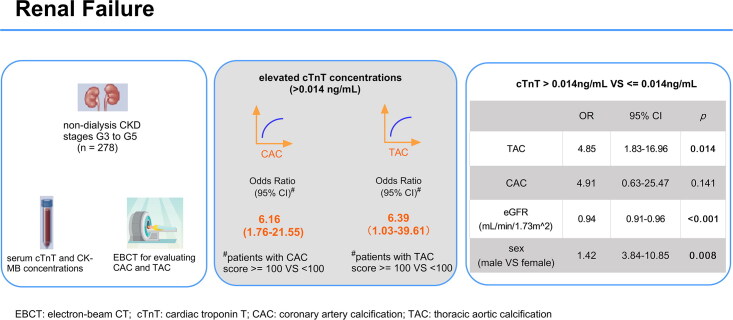
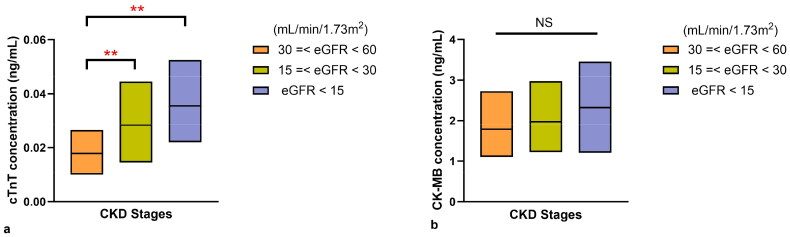
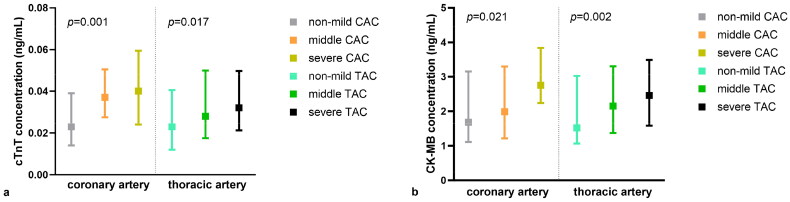
In 278 non-dialysis CKD patients of stage G3 to G5, we assessed calcified scores in CAC (Agatston score) and ECCs including thoracic aortic calcification (TAC), abdominal aortic calcification (AAC), carotid artery calcification, and valvular calcification. We analyzed the relationships between VC and myocardial injury markers of cardiac troponin T (cTnT) and creatine kinase-MB (CK-MB).
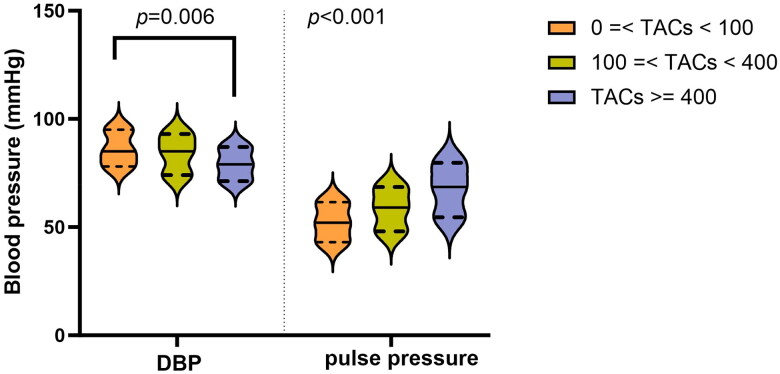
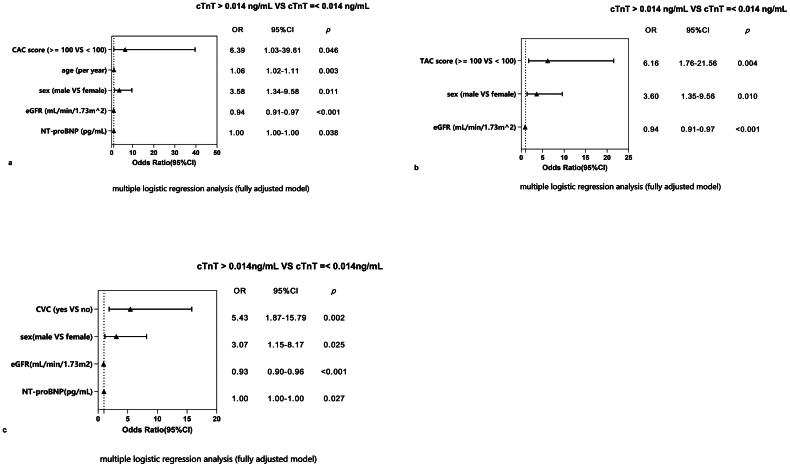
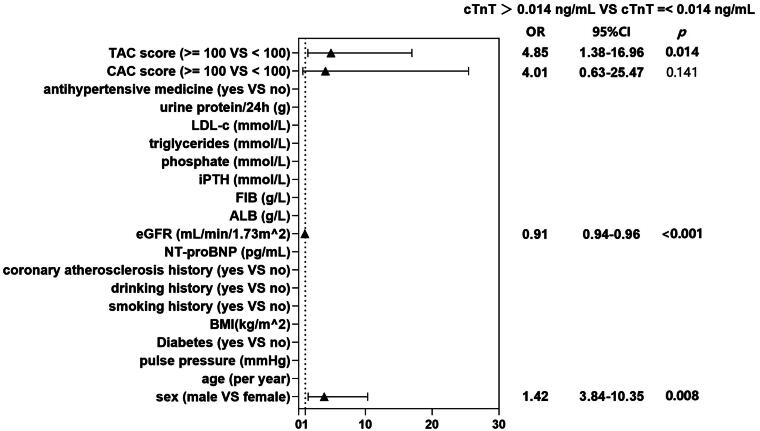
A total of 278 non-dialysis CKD patients (median age 52.4 ± 13.2; male 65.1%; diabetes 33.5%) were enrolled. A total of 71.8% (227) of patients had cTnT levels above the upper limit of normal (> 0.014 ng/mL). Moderate to severe (calcified score ≥100 vs. <100), CAC (OR 6.39; 95% CI 1.03-39.61) and TAC (OR 6.16; 95% CI 1.76-21.55) were significantly associated with higher cTnT concentrations after adjustment for confounders. Additionally, male sex and a lower eGFR were also associated with cTnT elevation. However, when we included CAC and TAC in one model, only moderate to severe TAC (OR 4.85; 95% CI 1.38-16.96) was a risk factor for cTnT elevation, but not CAC. Furthermore, patients with severer TAC presented lower diastolic blood pressure (DBP), wider pulse pressure ( < 0.001) and higher prevalence of left ventricular hypertrophy (LVH).
Moderate to severe thoracic aortic calcification (TAC score ≥ 100) is significantly associated with elevated cTnT concentrations in non-dialysis CKD patients of stage G3 to G5. The linkage may result from decreased coronary perfusion and relative myocardial ischemia.
血管钙化(VC),尤其是冠状动脉钙化(CAC),是慢性肾脏病(CKD)患者心血管死亡的有力预测指标。最近的研究表明,冠状动脉外钙化(ECCs)的存在会导致心血管疾病(CVD)。心肌损伤标志物升高可预测CKD患者的死亡风险,并与CVD相关。然而,在非透析CKD患者中,包括CAC和ECCs在内的VC与心肌损伤标志物之间的关系仍未得到探索。
在278例G3至G5期非透析CKD患者中,我们评估了CAC(阿加斯顿评分)和ECCs的钙化评分,包括胸主动脉钙化(TAC)、腹主动脉钙化(AAC)、颈动脉钙化和瓣膜钙化。我们分析了VC与心肌肌钙蛋白T(cTnT)和肌酸激酶同工酶MB(CK-MB)这两种心肌损伤标志物之间的关系。
共纳入278例非透析CKD患者(中位年龄52.4±13.2岁;男性占65.1%;糖尿病患者占33.5%)。共有71.8%(227例)患者的cTnT水平高于正常上限(>0.014 ng/mL)。在对混杂因素进行调整后,中度至重度(钙化评分≥100 vs.<100)的CAC(比值比6.39;95%置信区间1.03-39.61)和TAC(比值比6.16;95%置信区间1.76-21.55)与较高的cTnT浓度显著相关。此外,男性和较低的估算肾小球滤过率(eGFR)也与cTnT升高有关。然而,当我们将CAC和TAC纳入一个模型时,只有中度至重度TAC(比值比4.85;95%置信区间1.38-16.96)是cTnT升高的危险因素,而CAC不是。此外,TAC更严重的患者舒张压(DBP)较低,脉压较宽(<0.001),左心室肥厚(LVH)的患病率较高。
在G3至G5期非透析CKD患者中,中度至重度胸主动脉钙化(TAC评分≥100)与cTnT浓度升高显著相关。这种联系可能是由于冠状动脉灌注减少和相对心肌缺血所致。