Zhang Yi, Zhou Hu, Suo Shanshan, Zhuang Junling, Yang Linhua, He Aili, Liu Qingchi, Du Xin, Gao Sujun, Li Yarong, Li Yan, Chen Yuqing, Wu Wen, Zhu Huanling, He Guangsheng, Hong Mei, Jiang Qian, Jiang Zhongxing, Jing Hongmei, Wang Jishi, Xu Na, Yue Lingling, Zheng Cuiping, Zhou Zeping, Jin Chenghao, Li Xin, Liu Lin, Xu Yajing, Wu Dengshu, Zhang Feng, Zhang Jin, Wu Liqing, Yin Hewen, Lv Binhua, Xiao Zhijian, Jin Jie
Department of Hematology, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, PR China.
Zhejiang Provincial Key Laboratory of Hematopoietic Malignancy, Zhejiang University, Hangzhou, PR China.
Blood Cancer J. 2024 Dec 18;14(1):216. doi: 10.1038/s41408-024-01202-8.
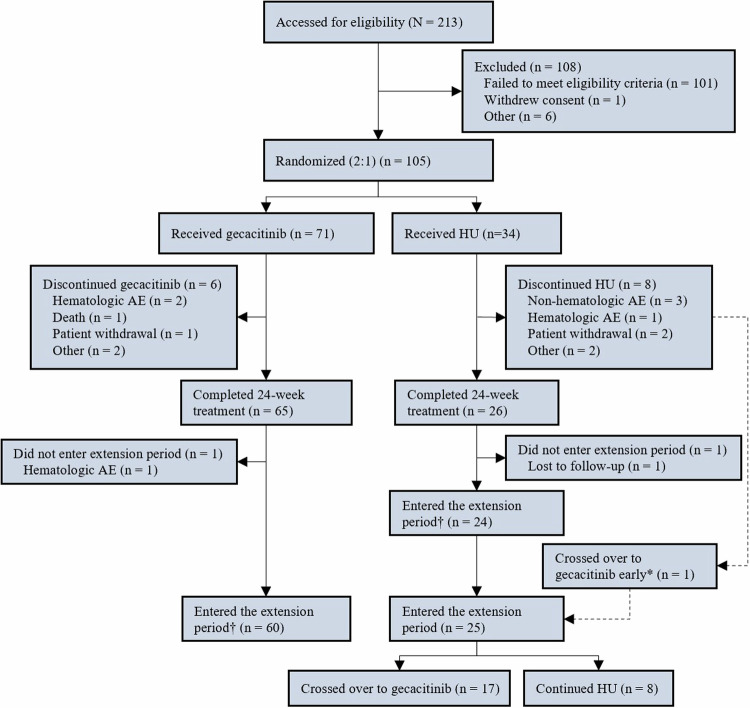
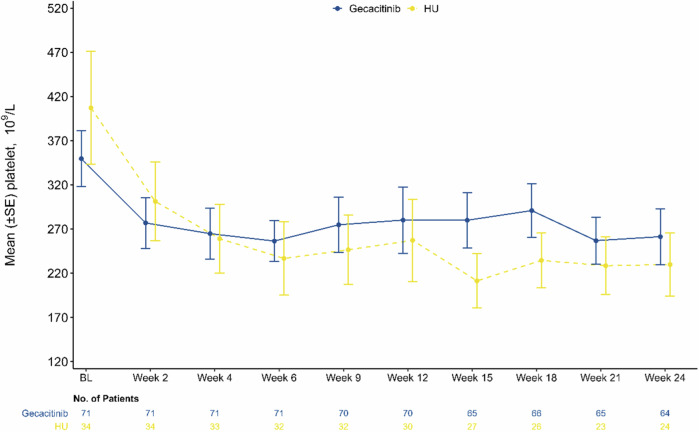
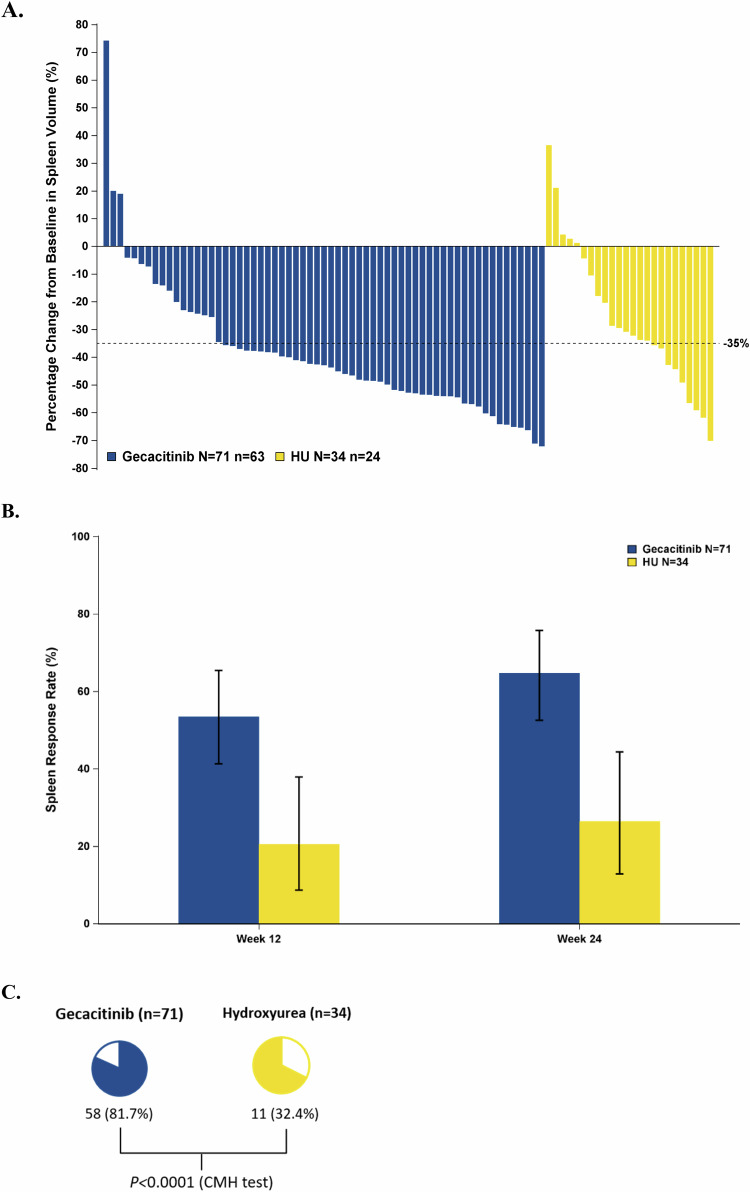
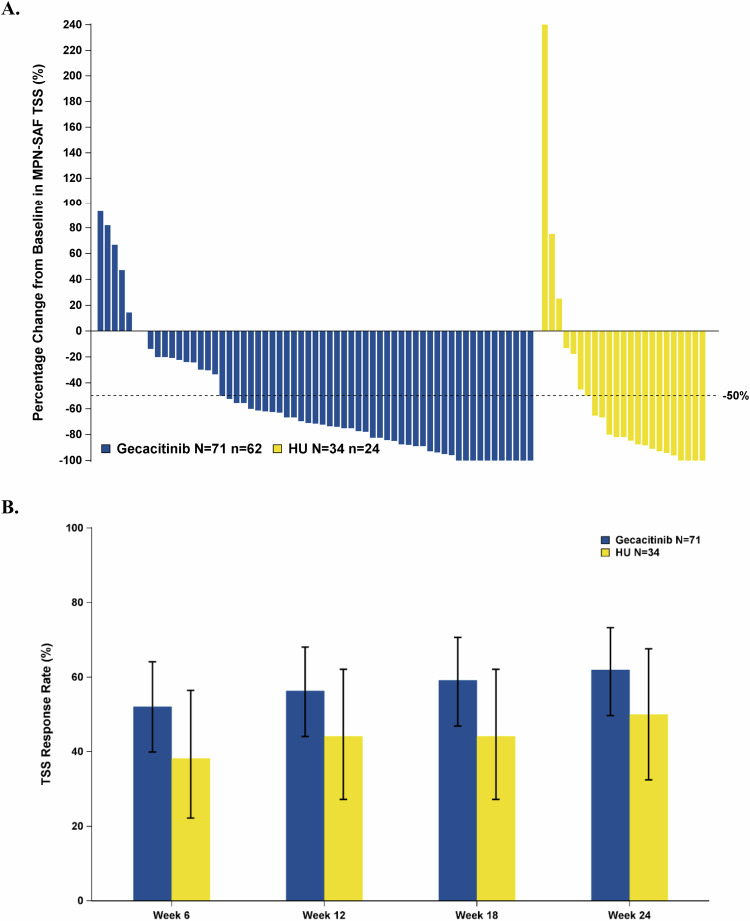
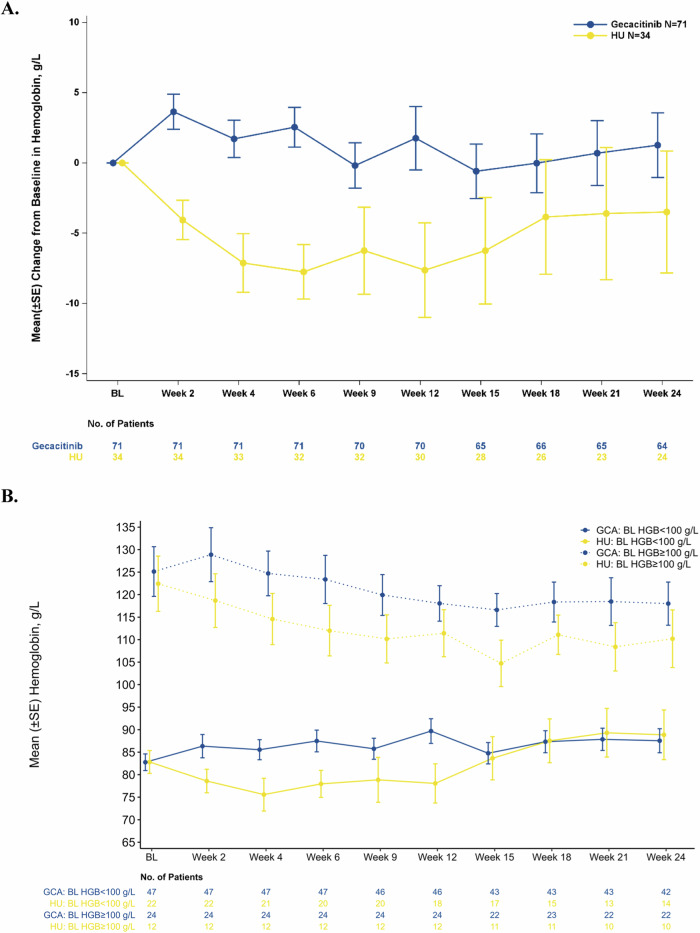
To compare the efficacy and safety of gecacitinib (also known as jaktinib) with hydroxyurea (HU) in treating myelofibrosis (MF) patients. In this multicenter, randomized phase 3 trial (ZGJAK016), intermediate- or high-risk primarily JAK inhibitor naïve MF patients were assigned in a 2:1 ratio to receive either gecacitinib (100 mg twice a day, BID) or HU (500 mg BID). The primary endpoint was the proportion of patients with ≥35% reduction in spleen volume (SVR35) from baseline at week 24. Secondary endpoints included the best spleen response rate, the proportion of patients with a ≥50% reduction in total symptom score (TSS50), anemia improvement, and safety profile. At 24 weeks, the SVR35 was reached by 64.8% of patients on gecacitinib (46/71), compared to 26.5% on HU (9/34), P = 0.0002. The best spleen response rates were also superior for gecacitinib at 81.7%, vs 32.4% for HU, P < 0.0001. The TSS50 rates were 62.0% for gecacitinib- and 50% for HU-treated patients. Among non-transfusion-dependent patients with baseline hemoglobin (HGB) ≤ 100 g/L, 31.0% (13/42) in the gecacitinib group showed a ≥20 g/L increase in HGB, compared to 15.0% (3/20) in HU group. The common grade ≥ 3 treatment-emergent adverse events (TEAEs), including anemia (26.8% vs 44.1%), thrombocytopenia (15.5% vs 32.4%), leukopenia (2.8% vs 20.6%), and neutropenia (1.4% vs 20.6%), were less frequent with gecacitinib than HU. Treatment discontinuation due to TEAEs was lower in gecacitinib (7.0%) compared to HU (11.8%). Gecacitinib demonstrates superior efficacy and a more favorable safety profile compared to HU, making it a promising treatment option for managing MF, particularly in patients with anemia (This trial was registered with ClinicalTrials.gov, (NCT04617028)).
比较吉卡替尼(也称为杰克替尼)与羟基脲(HU)治疗骨髓纤维化(MF)患者的疗效和安全性。在这项多中心、随机3期试验(ZGJAK016)中,将主要未使用过JAK抑制剂的中高危MF患者按2:1的比例分配,分别接受吉卡替尼(每日两次,每次100mg)或HU(每日两次,每次500mg)治疗。主要终点是第24周时脾脏体积较基线缩小≥35%(SVR35)的患者比例。次要终点包括最佳脾脏反应率、总症状评分降低≥50%(TSS50)的患者比例、贫血改善情况和安全性。在24周时,接受吉卡替尼治疗的患者中有64.8%(46/71)达到SVR35,而接受HU治疗的患者中这一比例为26.5%(9/34),P = 0.0002。吉卡替尼的最佳脾脏反应率也更高,为81.7%,而HU为32.4%,P < 0.0001。接受吉卡替尼和HU治疗的患者的TSS50率分别为62.0%和50%。在基线血红蛋白(HGB)≤100g/L的非输血依赖患者中,吉卡替尼组有31.0%(13/42)的患者HGB升高≥20g/L,而HU组为15.0%(3/20)。常见的≥3级治疗中出现的不良事件(TEAE),包括贫血(26.8%对44.1%)、血小板减少(15.5%对32.4%)、白细胞减少(2.8%对20.6%)和中性粒细胞减少(1.4%对20.6%),吉卡替尼组比HU组更少见。因TEAE导致的治疗中断率吉卡替尼组(7.0%)低于HU组(11.8%)。与HU相比,吉卡替尼显示出更好的疗效和更有利的安全性,使其成为治疗MF的有前景的选择,特别是对于贫血患者(本试验已在ClinicalTrials.gov注册,编号为NCT04617028)。