Saxena Amit, Sorrento Cristina, Izmirly Peter, Sullivan Janine, Gamez-Perez Monica, Law Jammie, Belmont Howard Michael, Buyon Jill P
Department of Medicine, Dvision of Rheumatology, NYU Grossman School of Medicine, New York City, New York, USA
Department of Medicine, Dvision of Rheumatology, NYU Grossman School of Medicine, New York City, New York, USA.
Lupus Sci Med. 2025 Jan 6;12(1):e001351. doi: 10.1136/lupus-2024-001351.
Traditional initial treatment regimens for lupus nephritis (LN) used oral glucocorticoids (GC) in starting doses up to 1.0 mg/kg/day prednisone equivalent with or without a preceding intravenous methylprednisolone pulse. More recent management guidelines recommend lower starting oral GC doses following intravenous pulse therapy. As there have been no large studies directly comparing patients receiving low versus high initial oral GC doses, this pooled analysis of high-quality randomised controlled trials (RCTs) aims to evaluate differences in efficacy and safety.
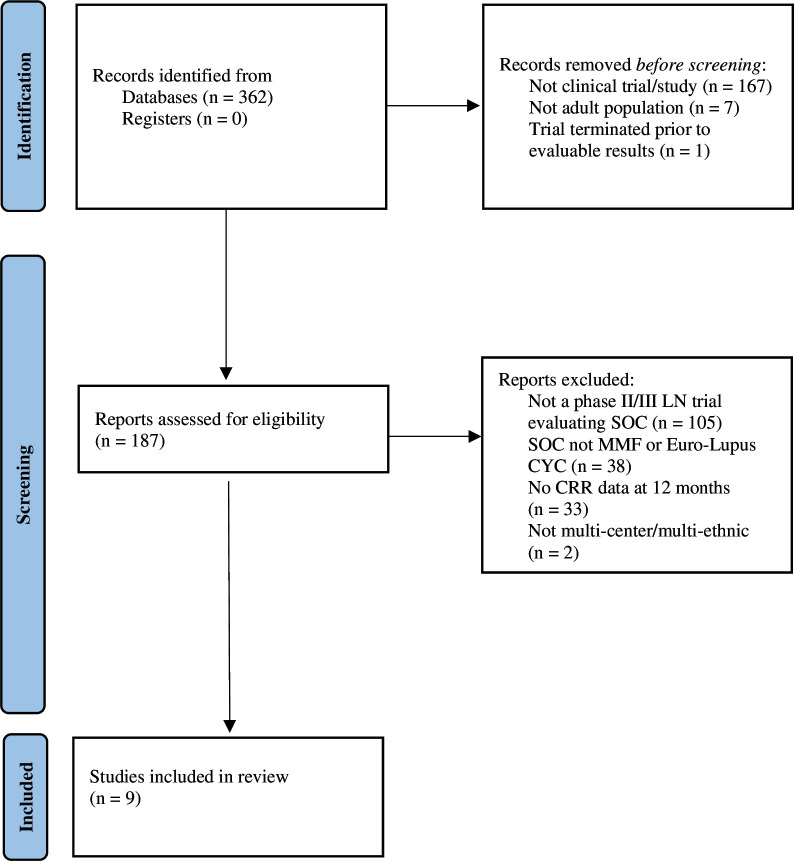
Published data were analysed from RCTs that assessed variable GC doses in the standard of care (SOC) treatment arms. Patients receiving starting prednisone doses up to 0.5 mg/kg/day (low dose) were compared with 1.0 mg/kg/day (high dose). Complete renal response requiring urine protein-creatinine ratio <0.5 mg/mg (CRR 0.5), CRR or partial renal response (PRR), serious adverse events (SAE) and SAE due to infections at 12 months of treatment were compared between groups.
417 patients from SOC arms of five studies were exposed to low-dose initial GC after intravenous pulse, while 521 patients from four studies were treated with high-dose oral GC. In patients with low-dose oral GC, 25.2% achieved CRR 0.5 at 12 months compared with 27.2% in high-dose groups, p=0.54. CRR or PRR was attained in 48.7% low-dose vs 43.6% high-dose patients, p=0.14. SAEs and infection SAEs were less common in the low-dose GC group (19.4% vs 31.6%, p<0.001 and 9.8% vs 16.5%, p=0.012, respectively).
Based on pooled RCT data, there was no significant difference in 12-month renal responses between patients receiving low-dose prednisone following intravenous GC compared with those receiving initial high doses. SAEs were less frequent in patients receiving low-dose initial GC. These findings support the use of lower oral GC doses in LN treatment.
狼疮性肾炎(LN)的传统初始治疗方案使用口服糖皮质激素(GC),起始剂量高达相当于每日1.0mg/kg的泼尼松,可联合或不联合前期静脉注射甲泼尼龙冲击治疗。最近的管理指南建议在静脉冲击治疗后降低口服GC的起始剂量。由于尚无大型研究直接比较接受低剂量与高剂量初始口服GC的患者,因此这项高质量随机对照试验(RCT)的汇总分析旨在评估疗效和安全性的差异。
分析已发表的RCT数据,这些试验评估了标准治疗(SOC)治疗组中不同的GC剂量。将接受起始泼尼松剂量高达每日0.5mg/kg(低剂量)的患者与每日1.0mg/kg(高剂量)的患者进行比较。比较两组在治疗12个月时达到尿蛋白-肌酐比值<0.5mg/mg的完全肾缓解(CRR 0.5)情况、CRR或部分肾缓解(PRR)情况、严重不良事件(SAE)以及因感染导致的SAE。
五项研究的SOC组中有417例患者在静脉冲击后接受低剂量初始GC治疗,而四项研究中有521例患者接受高剂量口服GC治疗。低剂量口服GC组中,25.2%的患者在12个月时达到CRR 0.5,高剂量组为27.2%,p=0.54。低剂量组48.7%的患者达到CRR或PRR,高剂量组为43.6%,p=0.14。SAE和感染性SAE在低剂量GC组中较少见(分别为19.4%对31.6%,p<0.001;9.8%对16.5%,p=0.012)。
基于汇总的RCT数据,与接受初始高剂量GC的患者相比,静脉注射GC后接受低剂量泼尼松治疗的患者在12个月时的肾脏反应无显著差异。接受低剂量初始GC治疗的患者SAE发生率较低。这些发现支持在LN治疗中使用较低剂量的口服GC。