Moreau Caroline, Odou Pascal, Labreuche Julien, Demailly Alexandre, Touzet Gustavo, Reyns Nicolas, Gouges Bastien, Duhamel Alain, Barthelemy Christine, Lannoy Damien, Carta Natacha, Palas Benjamin, Vasseur Michèle, Marchand Felix, Ollivier Thomas, Leclercq Céline, Potey Camille, Ouk Thavarak, Baigne Simon, Dujardin Kathy, Carton Louise, Rolland Anne Sophie, Devedjian Jean Christophe, Foutel Véronique, Deplanque Dominique, Fisichella Matthieu, Devos David
Parkinson's Disease Centre of Excellence, Department of Neurology, Univeristy of Lille, CHU Lille, INSERM U1172-Degenerative & Vascular Cognitive Disorders, Lille, France.
GRITA ULR 7365, University of Lille, Lille, France.
Nat Med. 2025 Mar;31(3):819-828. doi: 10.1038/s41591-024-03428-2. Epub 2025 Jan 7.
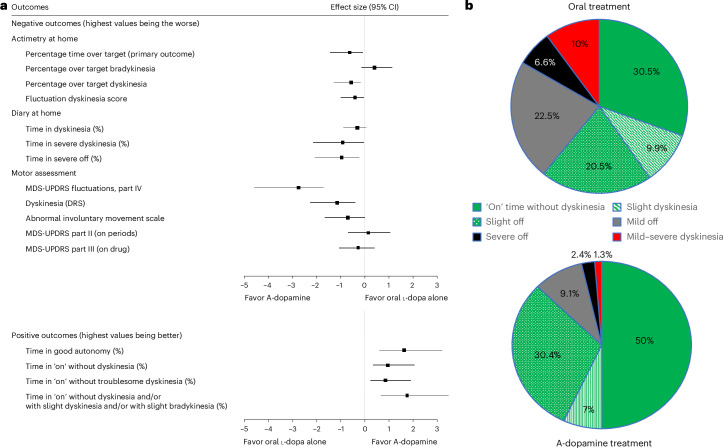
Continuous compensation for cerebral dopamine deficiency represents an ideal treatment for Parkinson's disease. Dopamine does not cross the digestive and blood-brain barriers and is rapidly oxidized. The new concept is the intracerebroventricular administration of anaerobic dopamine (A-dopamine) using an abdominal pump connected to a subcutaneous catheter implanted in the third ventricle, near the striatum. An open-label phase 1 study showed no serious adverse reactions induced by A-dopamine in 12 patients. A randomized, controlled, open-label, crossover phase 2 study of 1 month of A-dopamine versus 1 month of optimized oral antiparkinsonian therapy was conducted in 9 patients. The primary endpoint, a blinded assessment of the percentage over target (that is, time with dyskinesia or bradykinesia), recorded by home actimetry using a wristwatch, was significantly reduced on A-dopamine compared with that on oral treatment alone (P = 0.027), with a median within-patient difference of -10.4 (Hedge g = -0.62 (95% confidence interval: -1.43, -0.08)). Home diaries were also significantly improved. These initial data on the feasibility, safety and effects of this new device-assisted therapy suggest validation by a large randomized double-blind trial. ClinicalTrials.gov registration: NCT04332276 .
持续补偿大脑多巴胺缺乏是帕金森病的理想治疗方法。多巴胺不能穿过消化和血脑屏障,且会迅速被氧化。新的概念是使用连接到植入第三脑室(靠近纹状体)皮下导管的腹部泵进行厌氧多巴胺(A-多巴胺)的脑室内给药。一项开放标签的1期研究表明,12名患者使用A-多巴胺未引发严重不良反应。对9名患者进行了一项随机、对照、开放标签、交叉的2期研究,比较1个月的A-多巴胺与1个月的优化口服抗帕金森病治疗。主要终点是使用手表通过家庭活动计进行盲法评估的超过目标的百分比(即异动症或运动迟缓时间),与单独口服治疗相比,A-多巴胺治疗时该指标显著降低(P = 0.027),患者内差异中位数为-10.4(Hedge g = -0.62(95%置信区间:-1.43,-0.08))。家庭日记也有显著改善。这些关于这种新的设备辅助治疗的可行性、安全性和效果的初步数据表明,需要通过大型随机双盲试验进行验证。ClinicalTrials.gov注册编号:NCT04332276 。