Bánfi-Bacsárdi Fanni, Kazay Ádám, Gergely Tamás G, Forrai Zsolt, Füzesi Tamás Péter, Hanuska Laura Fanni, Schäffer Pál Péter, Pilecky Dávid, Vámos Máté, Vértes Vivien, Dékány Miklós, Andréka Péter, Piróth Zsolt, Nyolczas Noémi, Muk Balázs
Department of Adult Cardiology, Gottsegen National Cardiovascular Center, 1096 Budapest, Hungary.
Doctoral School of Clinical Medicine, University of Szeged, 6720 Szeged, Hungary.
J Clin Med. 2024 Dec 29;14(1):139. doi: 10.3390/jcm14010139.
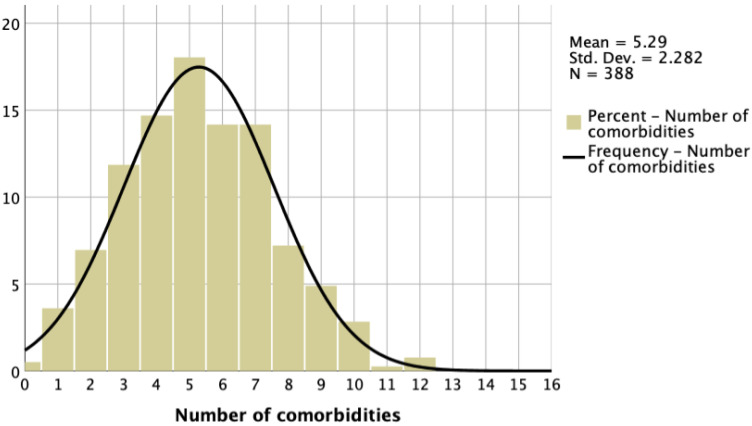
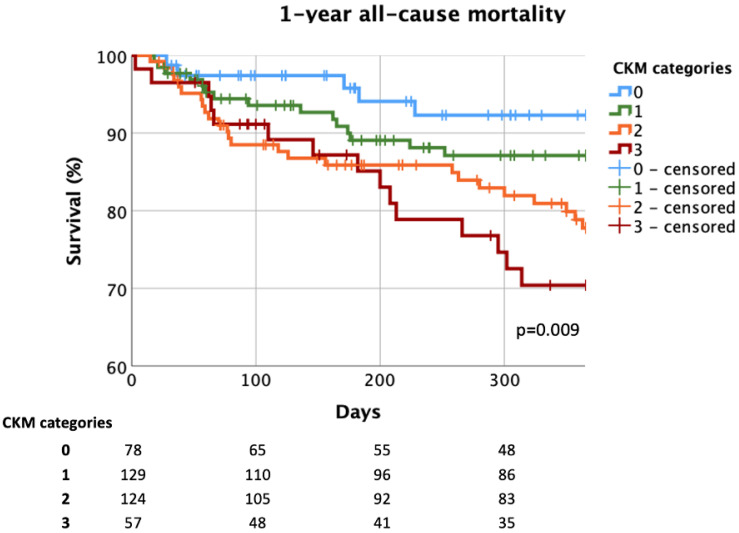
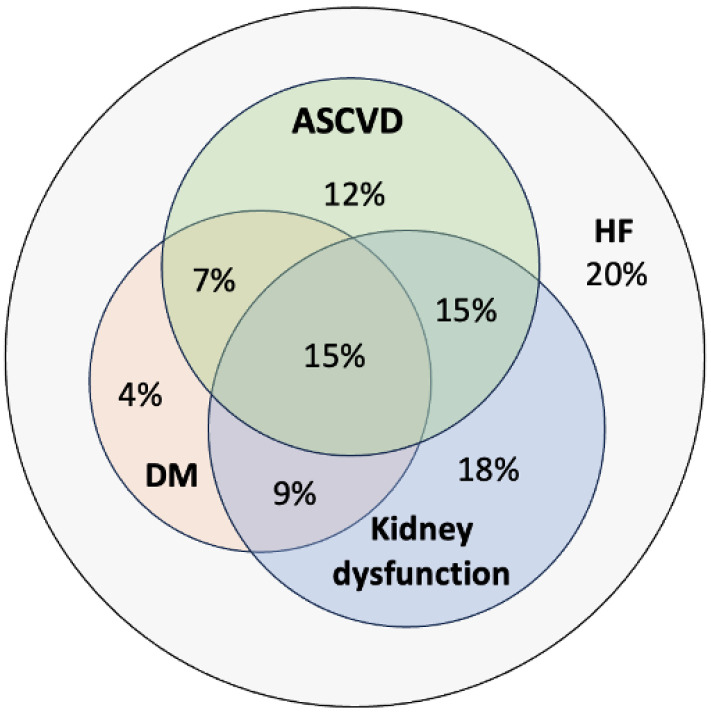
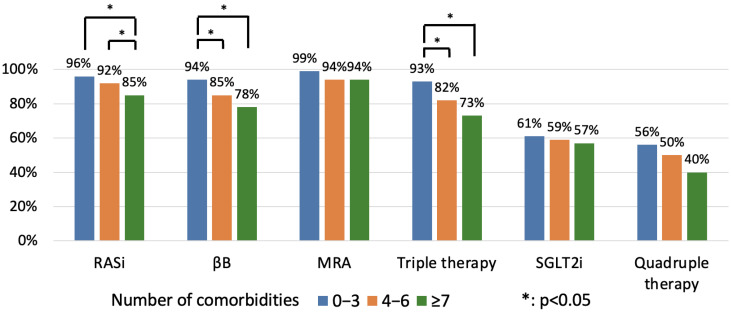
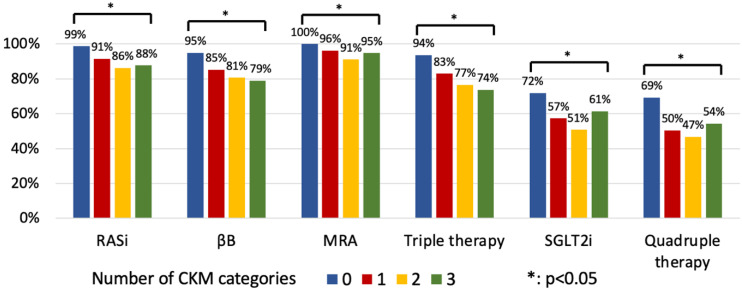
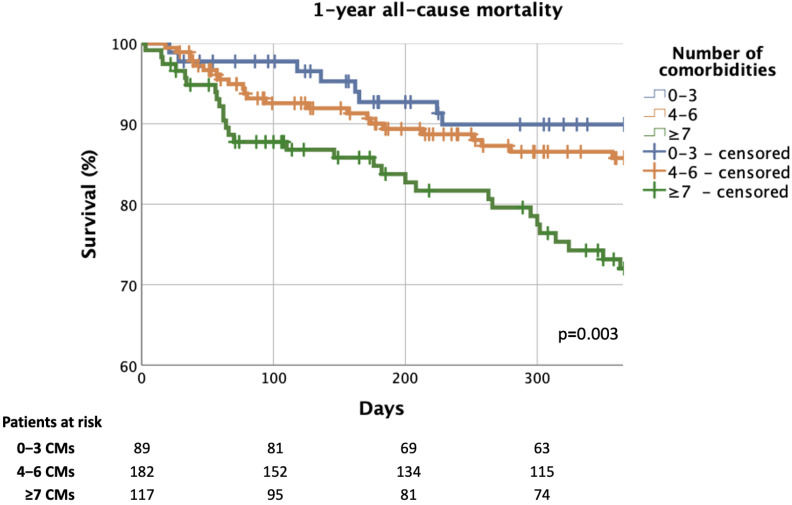
: In heart failure (HF) with reduced ejection fraction (HFrEF), the early diagnosis and proper treatment of comorbidities (CMs) are of fundamental relevance. Our aim was to assess the prevalence of CMs among real-world patients requiring hospitalisation for HFrEF and to investigate the effect of CMs on the implementation of guideline-directed medical therapy (GDMT) and on all-cause mortality (ACM). : The data of a consecutive HFrEF patient cohort hospitalised for HF between 2021 and 2024 were analysed retrospectively. Sixteen CMs (6 CV and 10 non-CV) were considered. Patients were divided into three categories: 0-3 vs. 4-6 vs. ≥7 CMs. GDMT at discharge and ACM were compared among CM categories. The predictors of 1-year ACM were also evaluated. : From the 388 patients (male: 76%, age: 61 [50-70] years; NT-proBNP: 5286 [2570-9923] pg/mL; ≥2 cardiovascular-kidney-metabolic disease overlap: 46%), a large proportion received GDMT (RASi: 91%; βB: 85%; MRA: 95%; SGLT2i: 59%; triple therapy [TT: RASi+βB+MRA]: 82%; quadruple therapy [QT: TT + SGLT2i]: 54%) at discharge. Multimorbidity was accompanied with a ( < 0.05) lower application ratio of RASi (96% vs. 92% vs. 85%; 0-3 vs. 4-6 vs. ≥7 CMs) and βB therapy (94% vs. 85% vs. 78%), while MRA (99% vs. 94% vs. 94%) and SGTL2i use (61% vs. 59% vs. 57%) did not differ ( > 0.05). Patients with multimorbidity were less likely to be treated with TT (93% vs. 82% vs. 73%, = 0.001), while no difference was detected in the implementation of QT (56% vs. 54% vs. 50%, = 0.685). The 1-year ACM of patients with an increased burden of CMs was higher (9% vs. 13% vs. 25%, = 0.003). The risk of 1-year ACM was favourably affected by the use of TT/QT and less severe left ventricular systolic dysfunction, while having ≥5 CMs had an unfavourable impact on prognosis. : According to our real-world analysis, HFrEF patients with an increased burden of CMs can expect a less favourable outcome. However, modern GDMT can even be applied in this patient population, resulting in a significantly improved prognosis. Thus, clinicians should insist on the early, conscious implementation of a prognosis-modifying drug regime in multimorbid HF patients as well.
在射血分数降低的心力衰竭(HFrEF)中,合并症(CMs)的早期诊断和恰当治疗至关重要。我们的目的是评估因HFrEF需住院治疗的真实世界患者中CMs的患病率,并研究CMs对指南指导的药物治疗(GDMT)实施情况及全因死亡率(ACM)的影响。:回顾性分析了2021年至2024年间因心力衰竭住院的连续HFrEF患者队列的数据。考虑了16种CMs(6种心血管相关和10种非心血管相关)。患者分为三类:0 - 3种CMs、4 - 6种CMs、≥7种CMs。比较了不同CMs类别出院时的GDMT情况及ACM。还评估了1年ACM的预测因素。:在388例患者中(男性:76%,年龄:61[50 - 70]岁;N末端脑钠肽前体:5286[2570 - 9923]pg/mL;≥2种心血管 - 肾脏 - 代谢疾病重叠:46%),很大一部分患者出院时接受了GDMT(肾素 - 血管紧张素系统抑制剂[RASi]:91%;β受体阻滞剂[βB]:85%;醛固酮受体拮抗剂[MRA]:95%;钠 - 葡萄糖协同转运蛋白2抑制剂[SGLT2i]:59%;三联疗法[TT:RASi + βB + MRA]:82%;四联疗法[QT:TT + SGLT2i]:54%)。合并症患者中,RASi(96%对92%对85%;0 - 3种CMs对4 - 6种CMs对≥7种CMs)和βB治疗(94%对85%对78%)的应用比例较低(P < 0.05),而MRA(99%对94%对94%)和SGLT2i的使用(61%对59%对57%)无差异(P > 0.05)。合并症患者接受TT治疗的可能性较小(93%对82%对73%,P = 0.001),而QT实施情况无差异(56%对54%对50%,P = 0.685)。CMs负担增加的患者1年ACM更高(9%对13%对25%,P = 0.003)。使用TT/QT和较轻的左心室收缩功能障碍对1年ACM风险有有利影响,而有≥5种CMs对预后有不利影响。:根据我们的真实世界分析,CMs负担增加的HFrEF患者预后可能较差。然而,现代GDMT甚至可应用于该患者群体,从而显著改善预后。因此,临床医生也应坚持在合并多种疾病的HF患者中尽早、有意识地实施改善预后的药物治疗方案。