Osei Isaac, Schmidt-Chanasit Jonas, Licciardi Paul V, Secka Ousman, D'Alessandro Umberto, Salaudeen Rasheed, Sarwar Golam, Clarke Ed, Mohammed Nuredin I, Nguyen Cattram, Greenwood Brian, Jansen Stephanie, Mackenzie Grant A
Medical Research Council Unit The Gambia at London School of Hygiene & Tropical Medicine, Banjul, the Gambia; Department of Disease Control, Faculty of Infectious and Tropical Diseases, London School of Hygiene & Tropical Medicine, London, UK.
Bernhard Nocht Institute for Tropical Medicine, Department of Arbovirology and Entomology, Hamburg, Germany.
Vaccine. 2025 Feb 15;47:126712. doi: 10.1016/j.vaccine.2025.126712. Epub 2025 Jan 10.
Because booster doses of pneumococcal conjugate vaccine (PCV) may be given at a similar time to yellow fever vaccine (YF), it is important to assess the immune response to YF when co-administered with PCV. This has been investigated during a reduced-dose PCV trial in The Gambia.
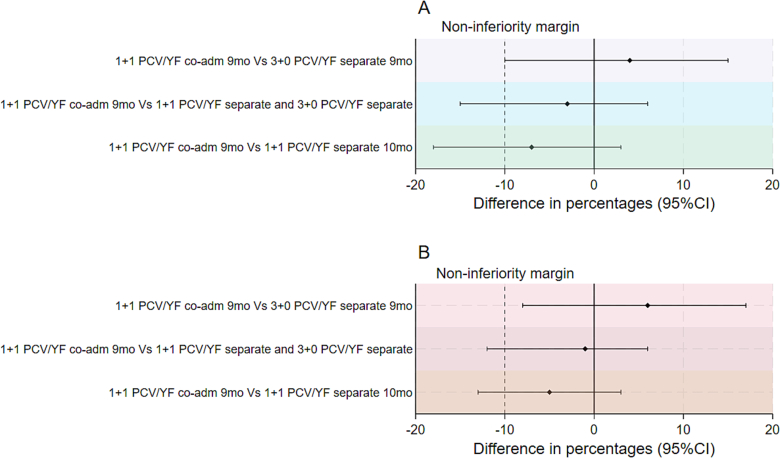
In this phase 4, parallel-group, cluster-randomized trial, healthy infants aged 0-10 weeks were randomly allocated to receive either a two-dose schedule of PCV13 with a booster dose co-administered with YF vaccine at age 9 months (1 + 1 co-administration) or YF vaccine administered separately at age 10 months (1 + 1 separate) or the standard three early doses of PCV13 with YF vaccine at age 9 months (3 + 0 separate). Blood samples were collected 28-35 days post-vaccination and YF neutralizing antibody (NA) titres were measured. Proportions with seroprotective YF NA titres ≥ 1:8 were calculated with 95 % confidence intervals (CI). Non-inferiority was demonstrated if the lower limit of the CI for the difference in proportions between the co-administration and separate groups was greater than - 10 %.
Forty-eight, 66, and 98 participants enrolled in 3 + 0 separate, 1 + 1 co-administration, and 1 + 1 separate groups respectively had NA results. Per protocol analysis of the 3 + 0 separate, 1 + 1 co-administration, 1 + 1 separate, and the combined 1 + 1 separate and 3 + 0 separate groups found that 81 %, 85 %, 92 %, and 88 % of participants respectively had YF NA titres ≥1:8. Results were similar with analysis by intention-to-treat. The difference in proportions comparing 1 + 1 co-administration and 1 + 1 separate groups was -7 % (95 % CI, -18 % to 3 %). The difference between 1 + 1 co-administration and 3 + 0 separate groups was 4 % (95 % CI, -10 % to 15 %). There was no statistical difference in the YF seroresponse when the YF vaccine was co-administered with PCV or administered separately.
No evidence was found of the non-inferiority of the seroresponse to YF vaccine when co-administered with PCV13. The levels of YF NA attaining seroprotection (NT ≥1:8) were high in all groups. PCV13 co-administered with YF vaccine at 9 months does not affect seroresponse to YF vaccine. http://www.isrctn.org/ - ISRCTN72821613.
由于肺炎球菌结合疫苗(PCV)的加强剂量可能与黄热病疫苗(YF)同时接种,因此评估与PCV联合接种时对YF的免疫反应非常重要。这已在冈比亚的一项低剂量PCV试验中进行了研究。
在这项4期、平行组、整群随机试验中,将0至10周龄的健康婴儿随机分配,分别接受两剂PCV13并在9个月龄时与YF疫苗同时接种加强剂量(1 + 1联合接种),或在10个月龄时单独接种YF疫苗(1 + 1分开接种),或标准的3剂早期PCV13并在9个月龄时接种YF疫苗(3 + 0分开接种)。在接种疫苗后28 - 35天采集血样,并测量YF中和抗体(NA)滴度。计算血清保护性YF NA滴度≥1:8的比例及其95%置信区间(CI)。如果联合接种组与分开接种组比例差异的CI下限大于 - 10%,则证明非劣效性。
分别有48、66和98名参与者纳入3 + 0分开接种组、1 + 1联合接种组和1 + 1分开接种组并获得NA结果。对3 + 0分开接种组、1 + 1联合接种组、1 + 1分开接种组以及1 + 1分开接种组合3 + 0分开接种组的合并组进行符合方案分析发现,分别有81%、85%、92%和88%的参与者YF NA滴度≥1:8。意向性分析结果相似。比较1 + 1联合接种组和1 + 1分开接种组的比例差异为 - 7%(95%CI, - 百分之18至3%)。1 + 1联合接种组与3 + 0分开接种组之间的差异为4%(95%CI, - 10%至15%)。当YF疫苗与PCV联合接种或分开接种时,YF血清反应无统计学差异。
未发现与PCV13联合接种时YF疫苗血清反应非劣效的证据。所有组中达到血清保护(NT≥1:8)的YF NA水平都很高。9个月龄时PCV13与YF疫苗联合接种不影响对YF疫苗的血清反应。http://www.isrctn.org/ - ISRCTN72821613