Perniola Simone, Bruno Dario, Di Mario Clara, Campobasso Denise, Calabretta Martina, Gessi Marco, Petricca Luca, Tolusso Barbara, Alivernini Stefano, Gremese Elisa
Immunology Research Core Facility, Gemelli Science and Technology Park (GSTeP), Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy.
Clinical Immunology Division, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy.
Clin Rheumatol. 2025 Mar;44(3):1019-1029. doi: 10.1007/s10067-025-07331-0. Epub 2025 Jan 22.
Regardless of remission status, residual pain (RP) might persist in rheumatoid arthritis (RA). The aim of this study was to characterize RP, its perception, and patient-dependent features and to evaluate its possible association with residual synovitis in patients with RA in remission.
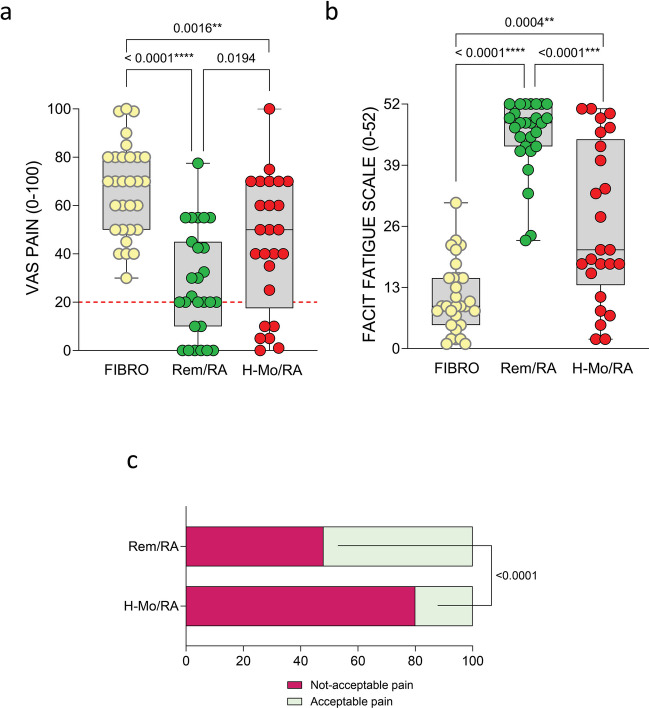
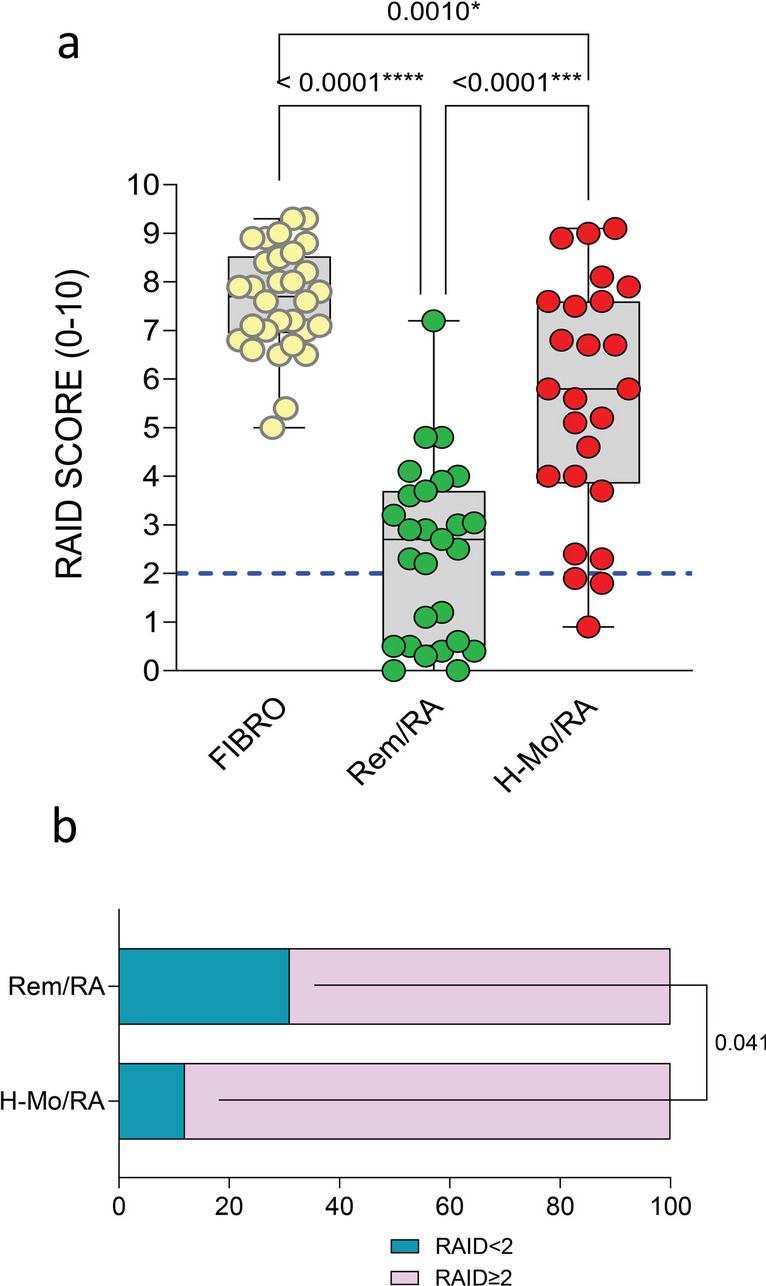
Ninety-seven patients with RA, including 68 in sustained clinical and ultrasound remission (Rem/RA) and 29 in high/moderate DAS28-CRP disease activity (H-Mo/RA) were enrolled in the study. Thirty patients with fibromyalgia were enrolled as a control group(FIBRO). At study entry, demographic, clinical, ultrasound characteristics, and pain dimension assessment (VAS-pain, FACIT, CSI, GHQ, and RAID) were collected for each patient. RA patients underwent synovial tissue biopsy to evaluate the degree of synovitis using the Krenn synovitis score (KSS).
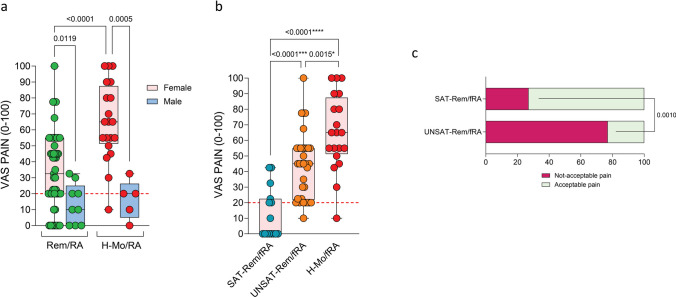
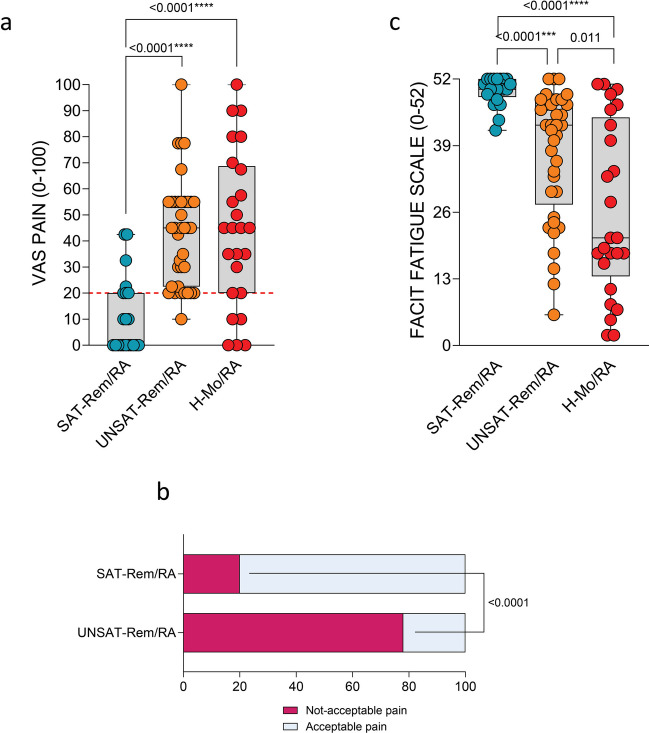
Forty-eight percent of Rem/RA still declared unacceptable pain (VAS-Pain > 20) compared to 80% of H-Mo/RA patients (p < 0.0001). Furthermore, Rem/RA patients presented comparable levels of pain dimension assessment regardless of KSS. However, classifying Rem/RA group based on RAID score (< 2 as satisfied SAT-Rem/RA and ≥ 2 as unsatisfied UNSAT-Rem/RA), SAT-Rem/RA group presented a lower grade of VAS-Pain (p < 0.0001), lower percentage of patients with an unacceptable pain (p < 0.0001) and lower grade of fatigue(p < 0.0001) compared to the UNSAT-Rem/RA patients. The percentage of SAT-Rem/RA patients who presented a disease flare did not differ from UNSAT-Rem/RA over the 24 months of follow-up. Finally, female Rem/RA patients presented higher VAS-Pain compared to male Rem/RA (p = 0.0119).
Moreover,73% satisfied female Rem/Ra patients presented an acceptable pain compared to 23% unsatisfied female Rem/RA patients (p = 0.001). RP in RA patients in remission can represent the way by which the patients communicate their state of non-acceptance of the disease. It can be useful to treat RP with the appropriate treatments. Key Points • Rheumatoid arthritis patients still reported unacceptable residual pain despite sustained clinical and ultrasound remission and despite the low grade/absence of histological synovitis. • Only a small rate of rheumatoid arthritis patients in sustained clinical and ultrasound remission showed residual pain as part of a central sensitivity syndrome or psychiatric disorders. • Rheumatoid arthritis patients in sustained clinical and ultrasound remission complained residual pain and fatigue as part of not acceptance of disease and/or dissatisfaction in the disease management.
无论缓解状态如何,类风湿关节炎(RA)患者可能仍存在残留疼痛(RP)。本研究的目的是描述RP及其认知、患者相关特征,并评估其与缓解期RA患者残留滑膜炎的可能关联。
97例RA患者纳入研究,其中68例处于持续临床和超声缓解状态(缓解/RA),29例处于高/中度DAS28-CRP疾病活动状态(高-中度/RA)。30例纤维肌痛患者作为对照组(纤维肌痛)。研究开始时,收集每位患者的人口统计学、临床、超声特征及疼痛维度评估(视觉模拟评分法疼痛评分、功能性癌症治疗-通用量表、临床症状指数、一般健康问卷、类风湿关节炎影响指数)。RA患者接受滑膜组织活检,使用克伦滑膜炎评分(KSS)评估滑膜炎程度。
48%的缓解/RA患者仍称疼痛难以接受(视觉模拟评分法疼痛评分>20),而高-中度/RA患者中这一比例为80%(p<0.0001)。此外,无论KSS如何,缓解/RA患者的疼痛维度评估水平相当。然而,根据类风湿关节炎影响指数评分(<2分为满意的SAT-缓解/RA,≥2分为不满意的UNSAT-缓解/RA)对缓解/RA组进行分类,与UNSAT-缓解/RA患者相比,SAT-缓解/RA组的视觉模拟评分法疼痛评分更低(p<0.0001),疼痛难以接受的患者百分比更低(p<0.0001),疲劳程度更低(p<0.0001)。在24个月的随访中,SAT-缓解/RA患者出现疾病复发的百分比与UNSAT-缓解/RA患者无差异。最后,女性缓解/RA患者的视觉模拟评分法疼痛评分高于男性缓解/RA患者(p=0.0119)。
此外,73%满意的女性缓解/RA患者疼痛可接受,而23%不满意的女性缓解/RA患者则不然(p=0.001)。缓解期RA患者的RP可能代表患者传达其对疾病不接受状态的方式。采用适当治疗方法治疗RP可能会有帮助。要点:• 类风湿关节炎患者尽管处于持续临床和超声缓解状态,且组织学滑膜炎程度低/无,但仍报告有难以接受的残留疼痛。• 只有一小部分处于持续临床和超声缓解状态的类风湿关节炎患者表现出残留疼痛是中枢性敏感综合征或精神障碍的一部分。• 处于持续临床和超声缓解状态的类风湿关节炎患者抱怨残留疼痛和疲劳是对疾病不接受和/或对疾病管理不满意的一部分。