Yang Yan, Li Xiao-Jin, Yuan Hua-Yan, Xiong Jing-Jing, Li Peng-Fei, Wang Zhen
Department of Intensive Care Medicine, Army Medical Center of PLA, No. 10 Changjiang Road, Yuzhong District, Chongqing, 400010, People's Republic of China.
Department of Neurology, Nanchuan Hospital Affiliated to Chongqing Medical University, 16 South Street, Nanchuan District, Chongqing, China.
BMC Pregnancy Childbirth. 2025 Jan 30;25(1):93. doi: 10.1186/s12884-025-07212-z.
Pregnancy-associated atypical hemolytic uremic syndrome (aHUS) is a form of thrombotic microangiopathy (TMA) caused by uncontrolled activation of the complement system during pregnancy or the postpartum period. In the intensive care unit, aHUS must be differentiated from sepsis-related multiple organ dysfunction, thrombotic thrombocytopenic purpura (TTP), hemolysis, elevated liver enzymes, and low platelet (HELLP) syndrome. Early recognition of aHUS is critical for effective treatment and improved prognosis. Although tests such as the ADAMTS13 level, peripheral blood smears, complement testing, and blood cultures are useful for diagnosing aHUS, these tests are time-consuming and may not be widely available. This report describes a case of severe aHUS in a pregnant woman during the coronavirus disease 2019 (COVID-19) pandemic.
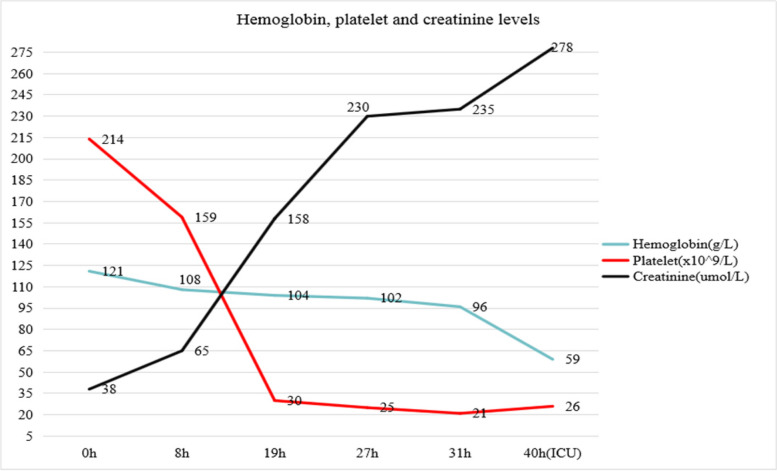
A 26-year-old patient with a history of four pregnancies and one delivery (P4G1) presented at 30 weeks and 2 days of gestation with vaginal fluid leakage and fetal growth restriction detected by ultrasound at a different hospital. During labor induction, the patient developed a high fever and coagulopathy, followed by heart failure, acute kidney injury, anemia, and severe thrombocytopenia. The patient remained alert and coherent, with no evidence of neurological dysfunction. She was transferred to our department and was given invasive respiratory support, blood transfusion, continuous renal replacement therapy, capacity management, and other comprehensive treatments. Due to the ongoing COVID-19 pandemic, ADAMTS13 testing and complement inhibitor therapy were unavailable. A diagnosis of pregnancy-associated aHUS was made based on the patient's history, clinical presentation, and standard laboratory results. The patient was prescribed 13 sessions of hemodialysis. Post-treatment evaluation showed normalized complement C3 and C4 levels, stabilized platelet and hemoglobin levels, and gradual normalization of liver function. Renal function improved gradually, and a bone marrow biopsy revealed no fragmented red blood cells. The patient was transferred to the Department of Nephrology on day 40 and back to the local hospital on day 42. The patient was followed up for 3 years, during which her renal function returned to normal, with no recurrence of thrombocytopenia or microangiopathic hemolytic anemia.
This case highlights the challenges and importance of diagnosing and managing pregnancy-associated aHUS and multiple organ failure in a low-resource setting.
妊娠相关非典型溶血性尿毒症综合征(aHUS)是一种血栓性微血管病(TMA),由妊娠期间或产后补体系统不受控制的激活引起。在重症监护病房,aHUS必须与脓毒症相关的多器官功能障碍、血栓性血小板减少性紫癜(TTP)、溶血、肝酶升高和血小板减少(HELLP)综合征相鉴别。早期识别aHUS对于有效治疗和改善预后至关重要。尽管诸如ADAMTS13水平检测、外周血涂片、补体检测和血培养等检查对诊断aHUS有用,但这些检查耗时且可能无法广泛开展。本报告描述了1例在2019冠状病毒病(COVID-19)大流行期间的孕妇严重aHUS病例。
一名有4次妊娠和1次分娩史(P4G1)的26岁患者,在妊娠30周零2天时因阴道流液就诊于另一家医院,超声检查发现胎儿生长受限。引产过程中,患者出现高热和凝血病,随后出现心力衰竭、急性肾损伤、贫血和严重血小板减少。患者神志清醒,无神经功能障碍迹象。她被转至我科,接受了有创呼吸支持、输血、持续肾脏替代治疗、容量管理及其他综合治疗。由于COVID-19大流行仍在持续,无法进行ADAMTS13检测和补体抑制剂治疗。根据患者病史、临床表现和标准实验室检查结果,诊断为妊娠相关aHUS。患者接受了13次血液透析治疗。治疗后评估显示补体C3和C4水平恢复正常,血小板和血红蛋白水平稳定,肝功能逐渐恢复正常。肾功能逐渐改善,骨髓活检未发现破碎红细胞。患者于第40天转至肾病科,第42天转回当地医院。对患者进行了3年随访,在此期间其肾功能恢复正常,血小板减少症或微血管病性溶血性贫血未复发。
本病例突出了在资源有限的情况下诊断和管理妊娠相关aHUS及多器官功能衰竭的挑战和重要性。