Benhalima Katrien, Minschart Caro, Geerts Ina, Ameye Lieveke, Van Der Schueren Bart, Devlieger Roland, Bogaerts Annick, Mathieu Chantal
Department of Endocrinolgy, University Hospitals Leuven, Leuven, Belgium.
Department of Chronic Diseases and Metabolism, Clinical and Experimental Endocrinology, KU Leuven, Leuven, Belgium.
BMC Med. 2025 Mar 18;23(1):165. doi: 10.1186/s12916-025-03992-5.
The suitability of the United States National Academy of Medicine guidelines for gestational weight gain in women with gestational diabetes remains uncertain, raising global concerns. This study aimed to evaluate the association of gestational weight gain with pregnancy and birth outcomes and to determine optimal ranges for gestational weight gain per pre-pregnancy body mass index category in women with gestational diabetes.
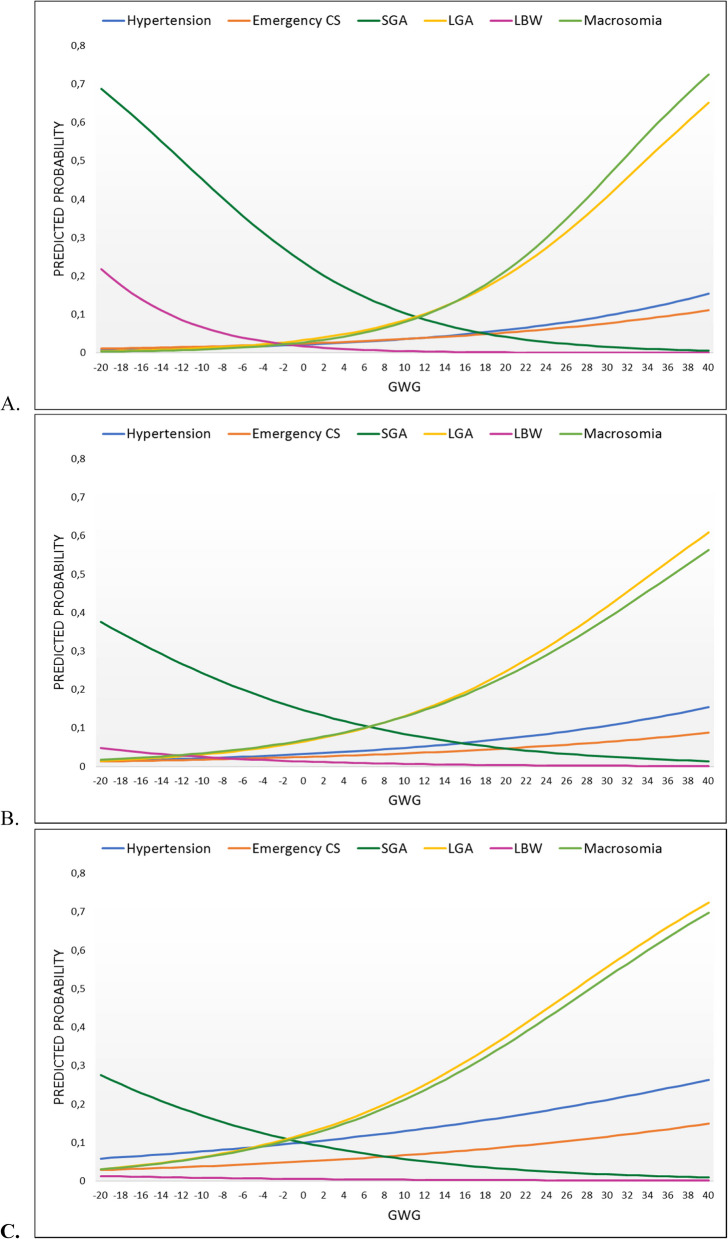
An epidemiological analysis between 2009-2018 analyzed a large Belgian cohort of singleton pregnancies with gestational diabetes and gestational age 38-40 weeks. Multivariate logistic regression assessed associations between gestational weight gain and relevant pregnancy and birth outcomes, with and without adjustment for confounding variables, including maternal age, origin, education, mode of conception, parity, gestational age at delivery, social deprivation, and year of delivery. Potential optimal weight gain ranges were calculated by minimizing the combined risk of small- and large-for-gestational-age infants (SGA, LGA).
A total of 13,060 women with gestational diabetes were included. Compared to recommended weight gain, gestational weight gain above guidelines occurred in 26.9% and was associated with an increased risk of gestational hypertension (aOR 1.41, 95% CI 1.20-1.66, p < 0.001), emergency caesarean section (aOR 1.45, 95% CI 1.25-1.69, p < 0.001), LGA infants (aOR 1.84, 95% CI 1.63-2.08, p < 0.001), and macrosomia (aOR 1.78, 95% CI 1.55-2.04, p < 0.001). Weight gain less than recommended (40.2%) was associated with a decreased risk of gestational hypertension (aOR 0.81, 95% CI 0.69-0.96, p = 0.015), LGA infants (aOR 0.58, 95% CI 0.50-0.66, p < 0.001), and macrosomia (aOR 0.57, 95% CI 0.49-0.65, p < 0.001), but at the expense of an increased risk of SGA infants (aOR 1.68, 95% CI 1.45-1.96, p < 0.001) and low birth weight (aOR 2.28, 95% CI 1.57-3.32, p < 0.001). Based on current analysis, the optimal ranges for gestational weight gain would be 9 to 14 kg for women with a normal weight, 1 to 9 kg for women with overweight, and -7 to 1 kg for women with obesity.
This Belgian study suggests that optimal gestational weight gain for singleton at-term pregnancies complicated by gestational diabetes should be lower than current recommendations, highlighting the need to reevaluate gestational weight gain guidelines in this context.
美国医学科学院关于妊娠期糖尿病女性孕期体重增加的指南是否适用仍不确定,引发了全球关注。本研究旨在评估妊娠期体重增加与妊娠及分娩结局之间的关联,并确定妊娠期糖尿病女性根据孕前体重指数类别划分的最佳孕期体重增加范围。
2009年至2018年的一项流行病学分析,对一大群孕周为38至40周的患有妊娠期糖尿病的单胎妊娠比利时队列进行了分析。多因素逻辑回归评估了妊娠期体重增加与相关妊娠及分娩结局之间的关联,同时对包括产妇年龄、出身、教育程度、受孕方式、产次、分娩时孕周、社会剥夺程度及分娩年份等混杂变量进行了调整和未调整的分析。通过最小化小于胎龄儿(SGA)和大于胎龄儿(LGA)的综合风险来计算潜在的最佳体重增加范围。
共纳入13060名妊娠期糖尿病女性。与推荐的体重增加相比,超过指南建议的妊娠期体重增加发生率为26.9%,并与妊娠期高血压风险增加相关(调整后比值比[aOR]为1.41,95%置信区间[CI]为1.20 - 1.66,p < 0.001)、急诊剖宫产(aOR为1.45,95% CI为1.25 - 1.69,p < 0.001)、LGA婴儿(aOR为1.84,95% CI为1.63 - 2.08,p < 0.001)及巨大儿(aOR为1.78,95% CI为1.55 - 2.04,p < 0.001)相关。体重增加低于推荐值(40.2%)与妊娠期高血压风险降低相关(aOR为0.81,95% CI为0.69 - 0.96,p = 0.015)、LGA婴儿(aOR为0.58,95% CI为0.50 - 0.66,p < 0.001)及巨大儿(aOR为0.57,95% CI为0.49 - 0.65,p < 0.001)相关,但代价是SGA婴儿风险增加(aOR为1.68,95% CI为1.45 - 1.96,p < 0.001)及低出生体重风险增加(aOR为2.28,95% CI为1.57 - 3.32, p < 0.001)。根据当前分析,正常体重女性的最佳孕期体重增加范围应为9至14千克,超重女性为1至9千克,肥胖女性为 - 7至1千克。
这项比利时研究表明,对于合并妊娠期糖尿病的单胎足月妊娠,最佳孕期体重增加应低于当前建议,凸显了在此背景下重新评估孕期体重增加指南的必要性。