Kim Minjoon, Lee Chaejin, Yoon Sang-Youl, Park Seong-Hyun, Hwang Jeong-Hyun, Kang Kyunghun, Park Eunhee, Choi Sunha, Lee Shin Yup, Yoo Seung Soo, Chae Yee Soo, Park Ki-Su
Department of Neurosurgery, School of Medicine, Kyungpook National University, 101 Dongin-dong 2 Ga, Jung-gu, Daegu, 700-422, Republic of Korea.
Department of Neurology, School of Medicine, Kyungpook National University, Daegu, Korea.
Acta Neurochir (Wien). 2025 Mar 19;167(1):81. doi: 10.1007/s00701-025-06490-y.
Leptomeningeal metastasis (LM)-associated hydrocephalus is a rare but severe complication of non-small cell lung cancer (NSCLC). The spread of malignant cells to the leptomeninges obstructs cerebrospinal fluid flow and increases intracranial pressure (ICP). This study compared the outcomes of lumboperitoneal (LP) and ventriculoperitoneal (VP) shunt surgeries in managing LM-associated hydrocephalus, focusing on symptom-free periods (SFPs) and overall survival (OS).
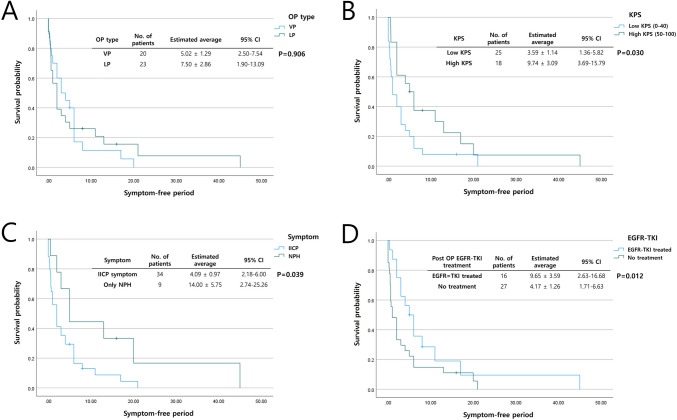
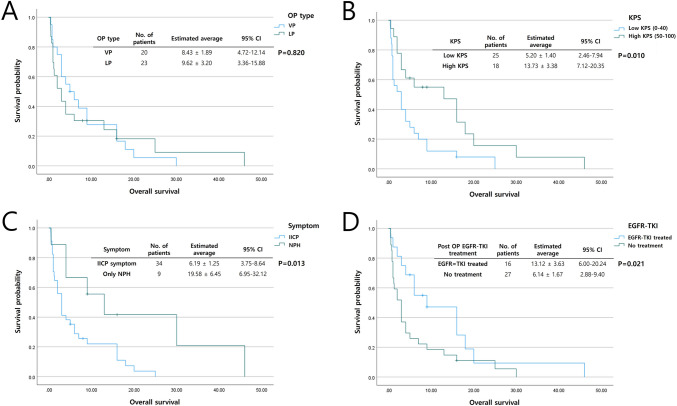
A retrospective analysis was conducted on 43 NSCLC patients with LM-associated hydrocephalus who underwent shunt surgery between 2017 and 2024. Patients were classified into LP (n = 23) and VP (n = 20) groups. Clinical characteristics, surgical outcomes, and survival rates were analyzed using Kaplan-Meier survival and Cox regression analyses. Karnofsky performance status (KPS), increased intracranial pressure (IICP) symptoms, and postoperative epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI) treatment were evaluated for prognostic significance.
No significant difference was observed between VP and LP shunt surgeries regarding SFP (VP: 5.02 ± 1.29 months, LP: 7.50 ± 2.86 months, p = 0.906) or OS (VP: 8.43 ± 1.89 months, LP: 9.62 ± 3.20 months, p = 0.820). High preoperative KPS, absence of ICP symptoms, and postoperative EGFR-TKI treatment were significantly associated with improved SFP and OS (p < 0.05). LP shunt surgery had shorter anesthesia and fewer complications compared to VP shunt surgery, representing a viable option for patients unsuitable for general anesthesia.
LP and VP shunt surgeries are equally effective for patients with LM-associated hydrocephalus in NSCLC. LP shunt surgery under local anesthesia could be recommended for its safety and patient acceptability. Favorable prognostic factors, including high KPS, absence of ICP, and postoperative EGFR-TKI treatment, should guide individualized treatment strategies to enhance patient outcomes and quality of life.
软脑膜转移(LM)相关的脑积水是一种罕见但严重的非小细胞肺癌(NSCLC)并发症。恶性细胞扩散至软脑膜会阻碍脑脊液流动并增加颅内压(ICP)。本研究比较了腰大池-腹腔(LP)分流术和脑室-腹腔(VP)分流术治疗LM相关脑积水的效果,重点关注无症状期(SFP)和总生存期(OS)。
对2017年至2024年间接受分流手术的43例NSCLC合并LM相关脑积水患者进行回顾性分析。患者分为LP组(n = 23)和VP组(n = 20)。采用Kaplan-Meier生存分析和Cox回归分析来分析临床特征、手术结果和生存率。评估卡诺夫斯基功能状态(KPS)、颅内压升高(IICP)症状以及术后表皮生长因子受体酪氨酸激酶抑制剂(EGFR-TKI)治疗的预后意义。
VP分流术和LP分流术在SFP(VP:5.02±1.29个月,LP:7.50±2.86个月,p = 0.906)或OS(VP:8.43±1.89个月,LP:9.62±3.20个月,p = 0.820)方面未观察到显著差异。术前KPS高、无ICP症状以及术后EGFR-TKI治疗与改善的SFP和OS显著相关(p < 0.05)。与VP分流术相比,LP分流术的麻醉时间更短且并发症更少,对于不适合全身麻醉的患者是一种可行的选择。
LP和VP分流术对NSCLC合并LM相关脑积水的患者同样有效。局部麻醉下的LP分流术因其安全性和患者可接受性值得推荐。包括高KPS、无ICP以及术后EGFR-TKI治疗在内的有利预后因素应指导个体化治疗策略,以提高患者的治疗效果和生活质量。