Jendoubi Ali, de Roux Quentin, Ribot Solène, Desauge Victor, Betbeder Tom, Picard Lucile, Ghaleh Bijan, Tissier Renaud, Kohlhauer Matthias, Mongardon Nicolas
Université Paris Est Créteil, INSERM, IMRB, Créteil, F-94010, France.
École Nationale Vétérinaire d'Alfort, IMRB, AfterROSC Network, Maisons-Alfort, F-94700, France.
Ann Intensive Care. 2025 Mar 19;15(1):32. doi: 10.1186/s13613-025-01458-8.
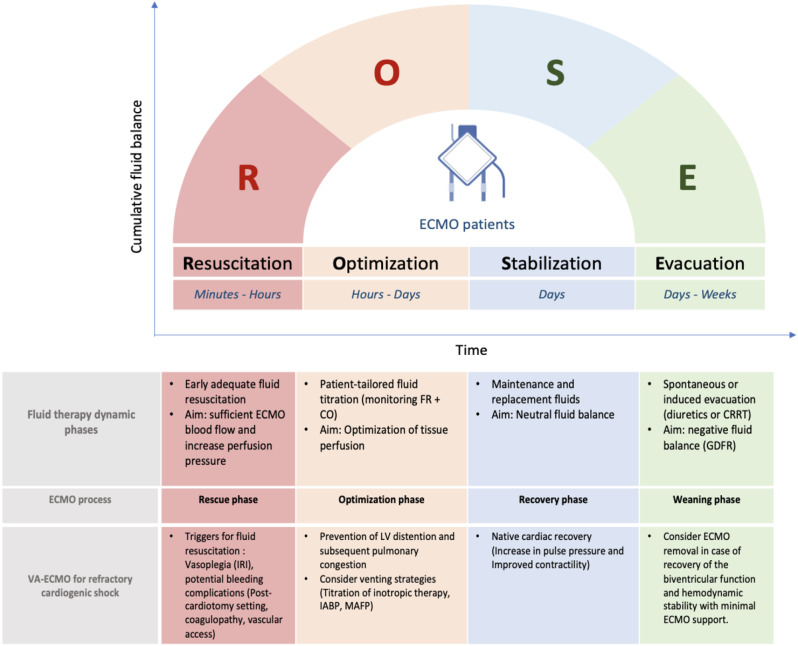
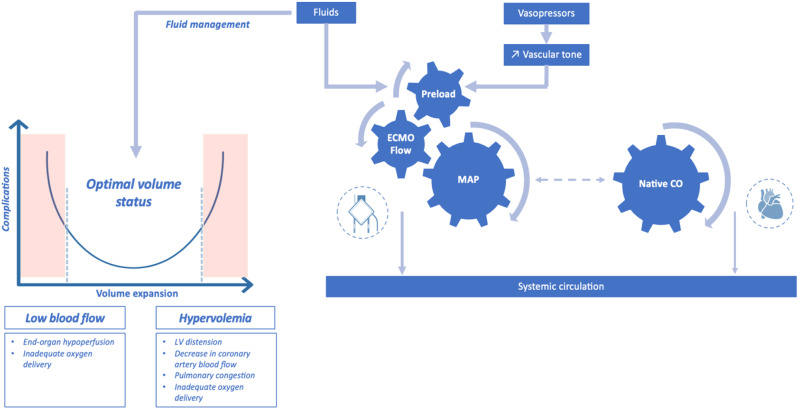
Venoarterial extracorporeal membrane oxygenation (VA-ECMO) offers an immediate and effective mechanical cardio-circulatory support for critically ill patients with refractory cardiogenic shock or selected refractory cardiac arrest. As fluid therapy is routinely performed as a component of initial hemodynamic resuscitation of ECMO supported patients, this narrative review intends to summarize the rationale and the evidence on the fluid resuscitation strategy in terms of fluid type and dosing, the impact of fluid balance on outcomes and fluid responsiveness assessment in VA-ECMO patients. Several observational studies have shown a deleterious impact of positive fluid balance on survival and renal outcomes. With regard to the type of crystalloids, further studies are needed to evaluate the safety and efficacy of saline versus balanced solutions in terms of hemodynamic stability, renal outcomes and survival in VA-ECMO setting. The place and the impact of albumin replacement, as a second-line option, should be investigated. During VA-ECMO run, the fluid management approach could be divided into four phases: rescue or salvage, optimization, stabilization, and evacuation or de-escalation. Echocardiographic assessment of stroke volume changes following a fluid challenge or provocative tests is the most used tool in clinical practice to predict fluid responsiveness. This review underscores the need for high-quality evidence regarding the optimal fluid strategy and the choice of fluid type in ECMO supported patients. Pending specific data, fluid therapy needs to be personalized and guided by dynamic hemodynamic approach coupled to close monitoring of daily weight and fluid balance in order to provide adequate ECMO flow and tissue perfusion while avoiding harmful effects of fluid overload.
静脉-动脉体外膜肺氧合(VA-ECMO)为患有难治性心源性休克或特定难治性心脏骤停的危重症患者提供即时且有效的机械性心肺循环支持。由于液体治疗是ECMO支持患者初始血流动力学复苏的常规组成部分,本叙述性综述旨在总结液体复苏策略在液体类型和剂量、液体平衡对结局的影响以及VA-ECMO患者液体反应性评估方面的基本原理和证据。多项观察性研究表明,正性液体平衡对生存和肾脏结局有有害影响。关于晶体液的类型,需要进一步研究以评估生理盐水与平衡液在VA-ECMO环境下对血流动力学稳定性、肾脏结局和生存方面的安全性和有效性。作为二线选择的白蛋白替代治疗的地位和影响也应进行研究。在VA-ECMO运行期间,液体管理方法可分为四个阶段:抢救或挽救、优化、稳定以及撤离或降级。在临床实践中,通过超声心动图评估液体负荷试验或激发试验后每搏输出量的变化是预测液体反应性最常用的工具。本综述强调了在ECMO支持的患者中,需要高质量证据来确定最佳液体策略和液体类型的选择。在缺乏具体数据的情况下,液体治疗需要个体化,并以动态血流动力学方法为指导,同时密切监测每日体重和液体平衡,以便在避免液体超负荷有害影响的同时提供足够的ECMO流量和组织灌注。