Nguyen Chi Phuong, Uyttenboogaart Maarten, Maas Willemijn J, Buskens Erik, Lahr Maarten M H, van der Zee Durk-Jouke
Department of Operations, Faculty of Economics and Business, University of Groningen, Groningen, The Netherlands
Health Technology Assessment, Department of Epidemiology, University Medical Center Groningen, Groningen, The Netherlands.
BMJ Open. 2025 Mar 29;15(3):e091413. doi: 10.1136/bmjopen-2024-091413.
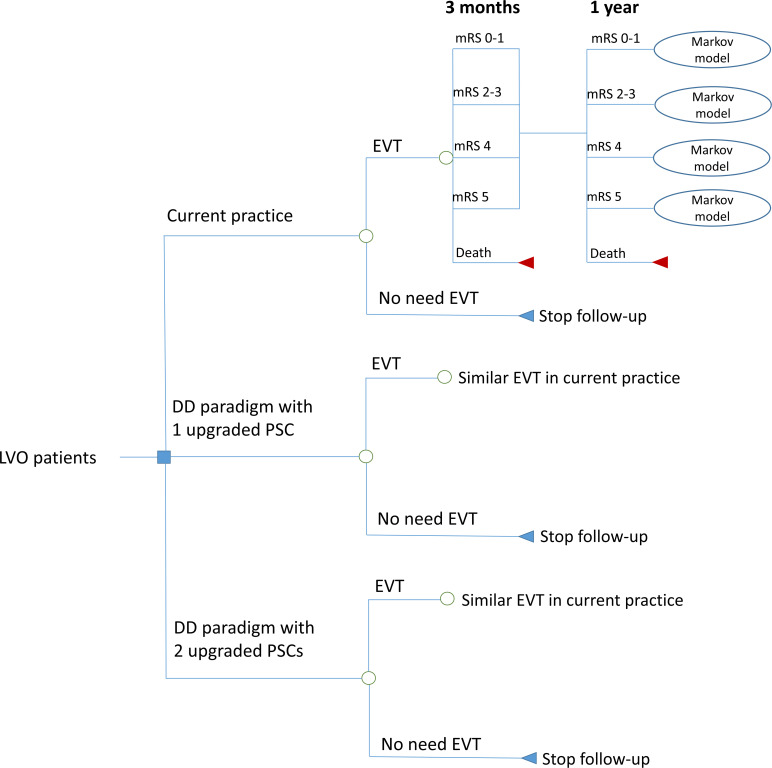
In a drive-the-doctor (DD) paradigm, an interventionalist travels from a comprehensive stroke centre (CSC) to primary stroke centres (PSCs) to perform endovascular thrombectomy (EVT) for acute ischaemic stroke due to large vessel occlusion (LVO). The DD paradigm may reduce time delays from onset to recanalisation. This study aimed to analyse the cost-effectiveness of the DD paradigm versus a drip-and-ship (DS) paradigm, where LVO patients are transferred from PSCs to a CSC for EVT in the northern Netherlands.
Economic evaluation was performed using a simulation model combined with a decision tree and a Markov model.
Stroke centres in the northern Netherlands.
A hypothetical cohort of 100 000 LVO patients with an average age of 70 years.
Two strategies were tested, including the DD paradigm with one upgraded PSC and the DD paradigm with two upgraded PSCs.
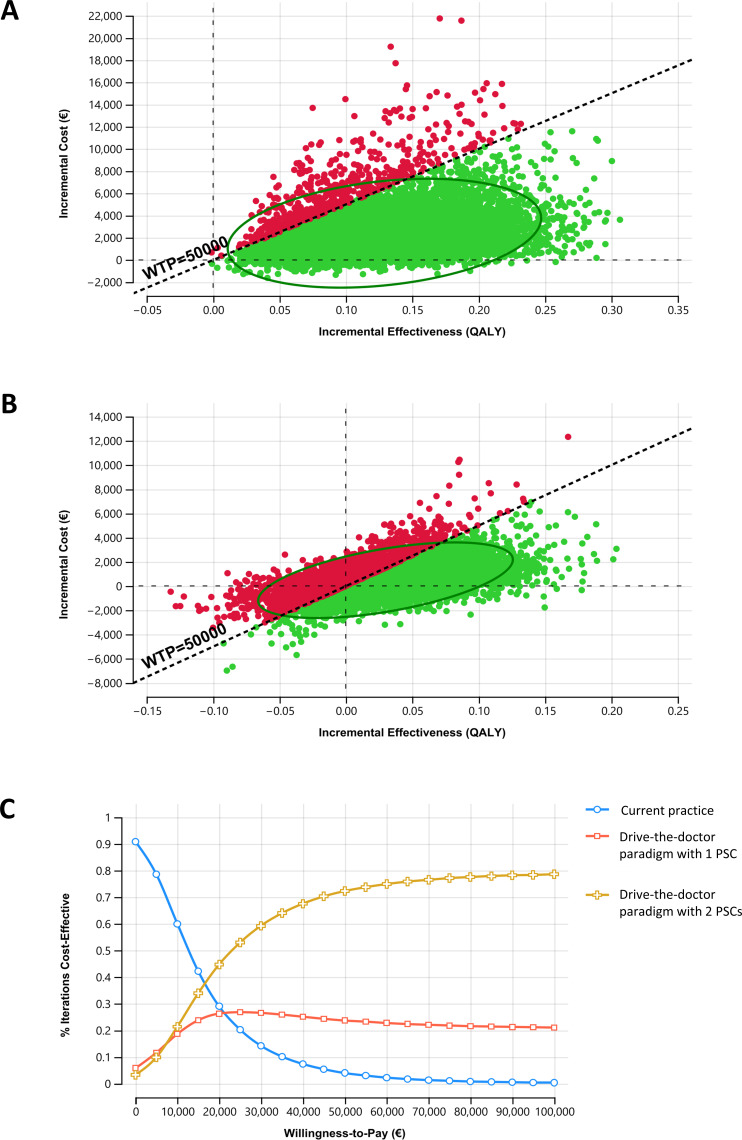
Total costs and quality-adjusted life years (QALYs) were measured over a 15-year time horizon from a Dutch healthcare provider perspective. An incremental cost-effectiveness ratio (ICER) of €50 000 was used as a willingness-to-pay threshold. One-way sensitivity, probabilistic sensitivity and scenario analyses (interventionalist transportation by car, ambulance and helicopter) were conducted to examine parameter uncertainty.
The DD paradigm using car as a transport modality and two PSCs was the optimal strategy, resulting in the lowest ICER. This strategy provided an additional 0.13 QALYs at incremental costs of €2367, yielding an ICER of €18 306 compared with current practice. The DD paradigm with two PSCs reduced ICERs compared with the scenario with one PSC when varying transportation modalities (car, ambulance and helicopter). Probabilistic sensitivity analyses showed that the DD paradigm with two PSCs using car was preferred in 72% of 10 000 Monte Carlo simulations.
The DD paradigm appeared cost-effective for LVO patients and may be considered a promising evolution for a regional stroke network.
在“驱动医生上门”(DD)模式中,介入专家从综合卒中中心(CSC)前往初级卒中中心(PSC),为因大血管闭塞(LVO)导致的急性缺血性卒中患者进行血管内血栓切除术(EVT)。DD模式可能会减少从发病到再通的时间延迟。本研究旨在分析DD模式与“点滴转运”(DS)模式的成本效益,在荷兰北部,LVO患者从PSC被转运至CSC进行EVT。
采用结合决策树和马尔可夫模型的模拟模型进行经济评估。
荷兰北部的卒中中心。
假设的100000名平均年龄为70岁的LVO患者队列。
测试了两种策略,包括配备一个升级PSC的DD模式和配备两个升级PSC的DD模式。
从荷兰医疗服务提供者的角度,在15年的时间范围内测量总成本和质量调整生命年(QALY)。以50000欧元的增量成本效益比(ICER)作为支付意愿阈值。进行单向敏感性分析、概率敏感性分析和情景分析(介入专家乘坐汽车、救护车和直升机运输)以检验参数不确定性。
使用汽车作为运输方式且配备两个PSC的DD模式是最优策略,产生的ICER最低。与当前实践相比,该策略以2367欧元的增量成本提供了额外的0.13个QALY,ICER为18306欧元。当改变运输方式(汽车、救护车和直升机)时,配备两个PSC的DD模式与配备一个PSC的情景相比降低了ICER。概率敏感性分析表明,在10000次蒙特卡洛模拟中,72%的模拟结果显示使用汽车的配备两个PSC的DD模式更优。
DD模式对LVO患者似乎具有成本效益,可能被视为区域卒中网络的一个有前景的发展方向。