Siriratnam Pakeeran, Huda Saif, Van der Walt Anneke, Sanfilippo Paul, Sharmin Sifat, Foong Yi Chao, Yeh Wei Zhen, Zhu Chao, Khoury Samia J, Csepany Tunde, Willekens Barbara, Etemadifar Masoud, Ozakbas Serkan, Nytrova Petra, Altintas Ayse, Al-Asmi Abdullah, Ramo-Tello Cristina, Laureys Guy, Patti Francesco, Horakova Dana, Foschi Matteo, Boz Cavit, McCombe Pamela, Turkoglu Recai, Roos Izanne, Lechner-Scott Jeannette, Kalincik Tomas, Jokubaitis Vilija, Butzkueven Helmut, Monif Mastura
Department of Neuroscience, Central Clinical School, Monash University, Melbourne, VIC, Australia.
Department of Neurology, Alfred Health, Melbourne, VIC, Australia.
J Neurol. 2025 Apr 14;272(5):339. doi: 10.1007/s00415-025-13064-6.
Previous studies have indicated that progression independent of relapse activity (PIRA) is uncommon in patients with aquaporin- 4 antibody-positive (AQP4-IgG) neuromyelitis optica spectrum disorder (NMOSD). However, the patterns of disability accumulation in seronegative NMOSD are unknown. This study aimed to evaluate the prevalence of PIRA and relapse-associated worsening (RAW) in seronegative NMOSD.
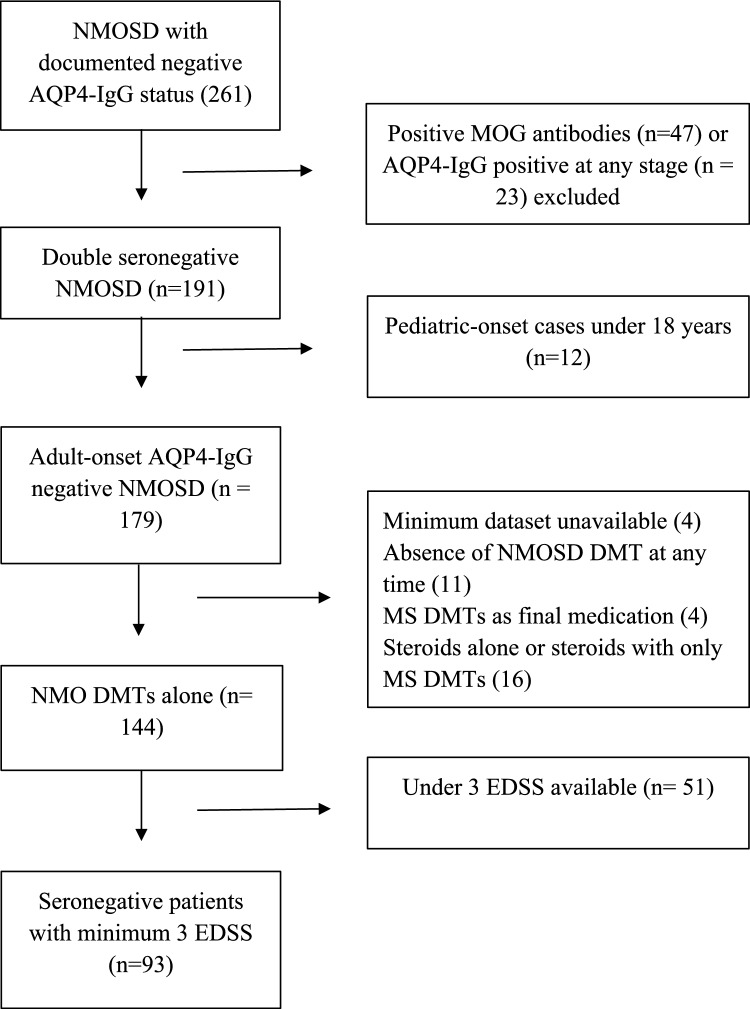
We conducted a retrospective, multicentre cohort study of seronegative NMOSD patients from the MSBase registry. Inclusion criteria required at least three recorded expanded disability status scale (EDSS) scores: baseline, progression, and 6 months confirmed disability progression (CDP). For those with 6-month CDP, the presence or absence of relapse between baseline and progression determined the classification as RAW or PIRA, respectively. Descriptive statistics were employed to present the data.
This study included 93 patients, with a median follow-up duration of 5.0 years (Q1 2.8, Q3 8.4). The cohort predominantly consisted of female patients (77.4%), with a median age of onset of 33.9 years (Q1 26.1, Q3 41.2). PIRA was observed in 1 case (1.1%), whilst RAW was documented in 7 cases (7.5%).
This international cohort study confirms that CDP is uncommon in seronegative NMOSD. Given more than three quarters of CDP occur due to RAW, therapeutic strategies should focus primarily on preventing relapses.
既往研究表明,水通道蛋白4抗体阳性(AQP4-IgG)的视神经脊髓炎谱系障碍(NMOSD)患者中,不依赖复发活动的病情进展(PIRA)并不常见。然而,血清学阴性的NMOSD患者的残疾累积模式尚不清楚。本研究旨在评估血清学阴性的NMOSD患者中PIRA和复发相关病情恶化(RAW)的发生率。
我们对MSBase注册中心的血清学阴性的NMOSD患者进行了一项回顾性、多中心队列研究。纳入标准要求至少记录三次扩展残疾状态量表(EDSS)评分:基线、病情进展和确认残疾进展(CDP)的6个月评分。对于有6个月CDP的患者,基线和病情进展之间是否存在复发分别决定了其分类为RAW或PIRA。采用描述性统计方法呈现数据。
本研究纳入了93例患者,中位随访时间为5.0年(第一四分位数2.8,第三四分位数8.4)。队列主要由女性患者组成(77.4%),中位发病年龄为33.9岁(第一四分位数26.1,第三四分位数41.2)。观察到1例PIRA(1.1%),同时记录到7例RAW(7.5%)。
这项国际队列研究证实,血清学阴性的NMOSD中CDP并不常见。鉴于超过四分之三的CDP是由RAW引起的,治疗策略应主要侧重于预防复发。